

Size matters: just how big is BIG?: Quantifying realistic sample size requirements for human genome epidemiology
- PMID: 18676414
- PMCID: PMC2639365
- DOI: 10.1093/ije/dyn147
Size matters: just how big is BIG?: Quantifying realistic sample size requirements for human genome epidemiology
Abstract
Background: Despite earlier doubts, a string of recent successes indicates that if sample sizes are large enough, it is possible-both in theory and in practice-to identify and replicate genetic associations with common complex diseases. But human genome epidemiology is expensive and, from a strategic perspective, it is still unclear what 'large enough' really means. This question has critical implications for governments, funding agencies, bioscientists and the tax-paying public. Difficult strategic decisions with imposing price tags and important opportunity costs must be taken.
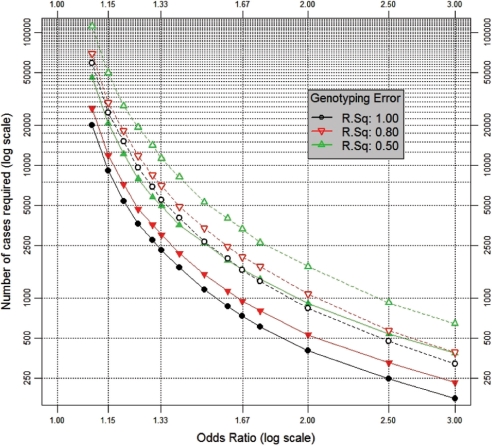
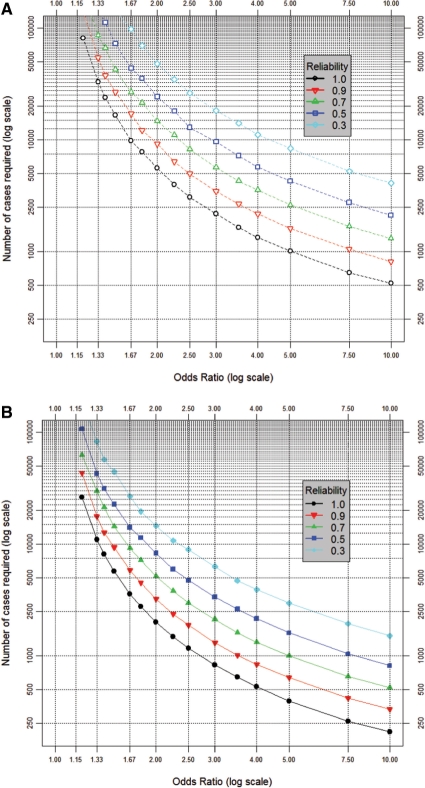
Methods: Conventional power calculations for case-control studies disregard many basic elements of analytic complexity-e.g. errors in clinical assessment, and the impact of unmeasured aetiological determinants-and can seriously underestimate true sample size requirements. This article describes, and applies, a rigorous simulation-based approach to power calculation that deals more comprehensively with analytic complexity and has been implemented on the web as ESPRESSO: (www.p3gobservatory.org/powercalculator.htm).
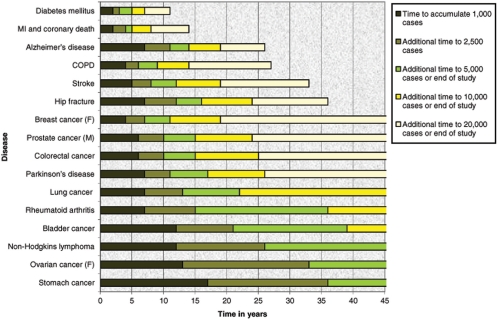
Results: Using this approach, the article explores the realistic power profile of stand-alone and nested case-control studies in a variety of settings and provides a robust quantitative foundation for determining the required sample size both of individual biobanks and of large disease-based consortia. Despite universal acknowledgment of the importance of large sample sizes, our results suggest that contemporary initiatives are still, at best, at the lower end of the range of desirable sample size. Insufficient power remains particularly problematic for studies exploring gene-gene or gene-environment interactions. Discussion Sample size calculation must be both accurate and realistic, and we must continue to strengthen national and international cooperation in the design, conduct, harmonization and integration of studies in human genome epidemiology.
Figures
Comment in
-
Commentary: How small is small?Int J Epidemiol. 2009 Feb;38(1):274-5. doi: 10.1093/ije/dyn232. Epub 2008 Nov 3. Int J Epidemiol. 2009. PMID: 18984600 No abstract available.
References
-
- World Health Organization (WHO) Geneva: Joint WHO/FAO Expert Consultation; 2005. Diet, Nutrition and the Prevention of Chronic Diseases. The Aethiology of these Diseases.
-
- O’Rahilly S, Wareham NJ. Genetic variants and common diseases–better late than never. N Engl J Med. 2006;355:306–8. - PubMed
-
- Lander ES. The new genomics: global views of biology. Science. 1996;274:536–39. - PubMed
-
- Cargill M, Daley GQ. Mining for SNPs: putting the common variants–common disease hypothesis to the test. Pharmacogenomics. 2000;1:27–37. - PubMed
-
- Reich DE, Lander ES. On the allelic spectrum of human disease. Trends Genet. 2001;17:502–10. - PubMed
