

Surgical management of unstable elbow dislocation without intra-articular fracture
- PMID: 18677481
- PMCID: PMC2898997
- DOI: 10.1007/s00264-008-0624-x
Surgical management of unstable elbow dislocation without intra-articular fracture
Abstract
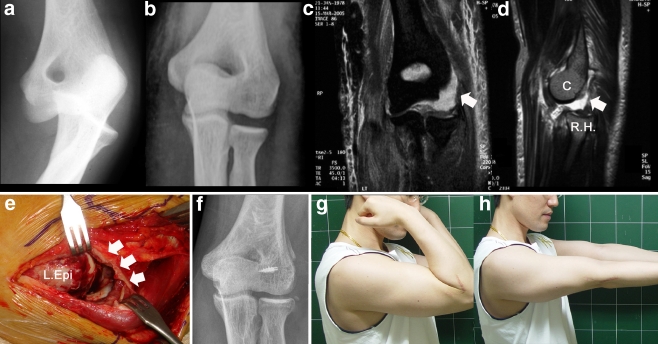
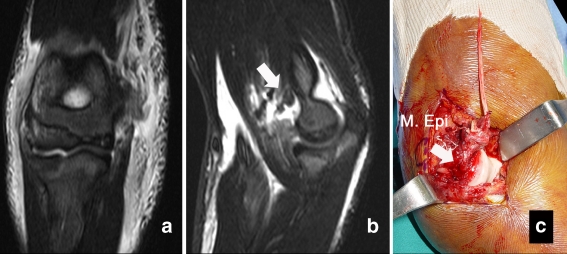
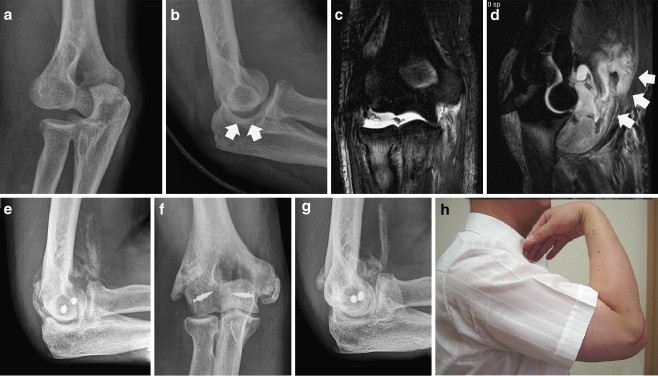
The purpose of this study was to describe soft tissue injury patterns and report the clinical results of primary ligament repair with use of protected early mobilisation in unstable elbow dislocations with pure capsulo-ligamentous injuries. Twenty-four patients who presented with traumatic unstable elbow dislocation without associated intra-articular fracture were reviewed. Anatomical repair was performed using metal anchor screws and the bone tunnel method. Ligament avulsion was noted in 55% for the medial collateral ligament, 80% for the lateral collateral ligament, 60% for the flexor tendon and 80% for the extensor tendon. The overall mean Mayo Elbow Performance Score was 93.2. Brachial artery injuries occurred in two elbows. Heterotopic calcification was noted in 14 patients and there was one severe traumatic arthrosis. This study showed a high incidence of reattachable avulsion injuries to ligaments, tendon/muscle and capsule in unstable elbow dislocations. Primary ligament repair coupled with early rehabilitation provided satisfactory outcomes at two to four years postoperatively.
Le but de cette étude est de décrire les lésions et de rapporter les résultats chez les patients présentant une luxation du coude avec lésion ligamentaire traitée par réparation ligamentaire et mobilisation précoce. Matériel et méthode: 24 patients présentant ce type de traumatisme sans lésion fracturaire intra articulaire ont été revus. Les lésions anatomiques ont été réparées avec soit une ancre soit une fixation ligamentaire par tunnels trans-osseux. Résultats: l’avulsion ligamentaire est notée dans 55% des cas pour le MCL, dans 80% pour le LCL, dans 60% pour le tendon fléchisseur et dans 80% dans le tendon extenseur. En tout état de cause, le score MEPS a été de 93,2. Une lésion de l’artère humérale a été observée sur deux coudes et des lésions de calcifications hétérotypiques ont été observées chez 14 patients avec, dans un cas, une arthrose sévère. Conclusion: cette étude montre l’influence que peut avoir la réinsertion ligamentaire dans ces lésions secondaires à une luxation du coude. Les réparations précoces associées à une réhabilitation également précoce permettent d’avoir des résultats satisfaisants après deux mois de suivi post-opératoire.
Figures
References
-
- Broberg MA, Morrey BF. Results of delayed excision of the radial head after fracture. J Bone Joint Surg Am. 1986;68:669–674. - PubMed
-
- Cohen MS, Hastings H., 2nd Acute elbow dislocation: evaluation and management. J Am Acad Orthop Surg. 1998;6:15–23. - PubMed
-
- Dryer RF, Buckwalter JA, Sprague BL. Treatment of chronic elbow instability. Clin Orthop Relat Res. 1980;148:254–255. - PubMed
-
- Dürig M, Müller W, Rüedi TP, Gauer EF. The operative treatment of elbow dislocation in the adult. J Bone Joint Surg Am. 1979;61:239–244. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
