

Mitral leaflet adaptation to ventricular remodeling: occurrence and adequacy in patients with functional mitral regurgitation
- PMID: 18678770
- PMCID: PMC2662377
- DOI: 10.1161/CIRCULATIONAHA.107.749440
Mitral leaflet adaptation to ventricular remodeling: occurrence and adequacy in patients with functional mitral regurgitation
Abstract
Background: Functional mitral regurgitation (MR) is caused by systolic traction on the mitral leaflets related to ventricular distortion. Little is known about whether chronic tethering causes the mitral leaflet area to adapt to the geometric needs imposed by tethering, in part because of inability to reconstruct leaflet area in vivo. Our aim was to explore whether adaptive increases in leaflet area occur in patients with functional MR compared with normal subjects and to test the hypothesis that leaflet area influences MR severity.
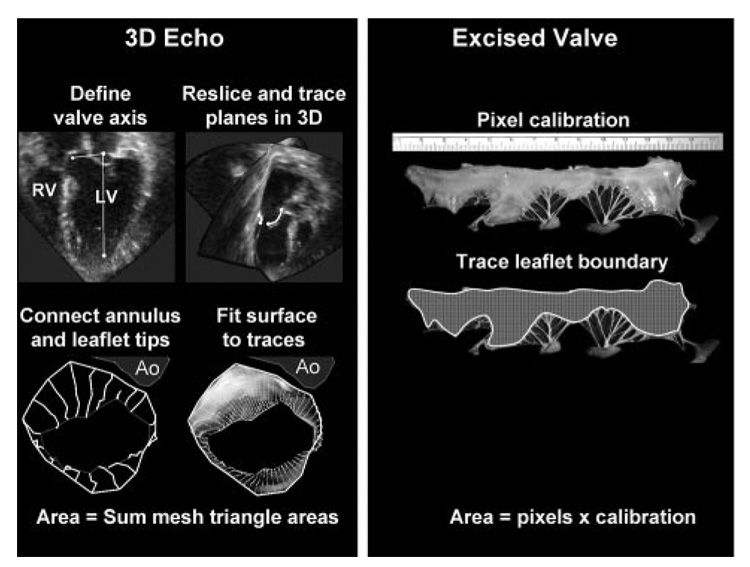
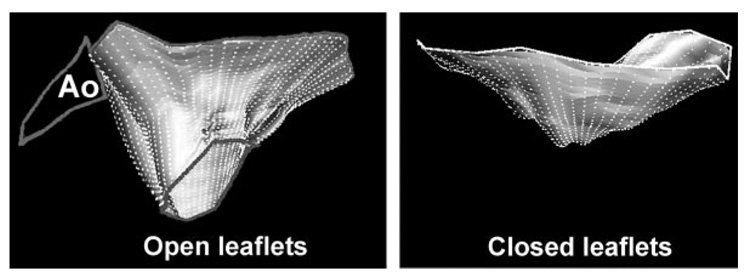
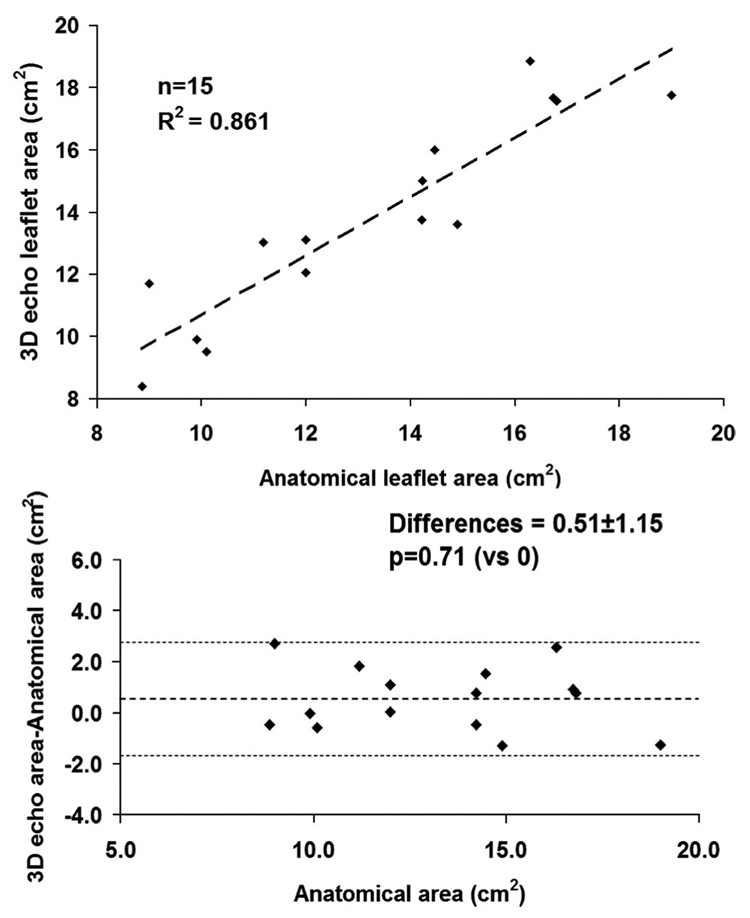
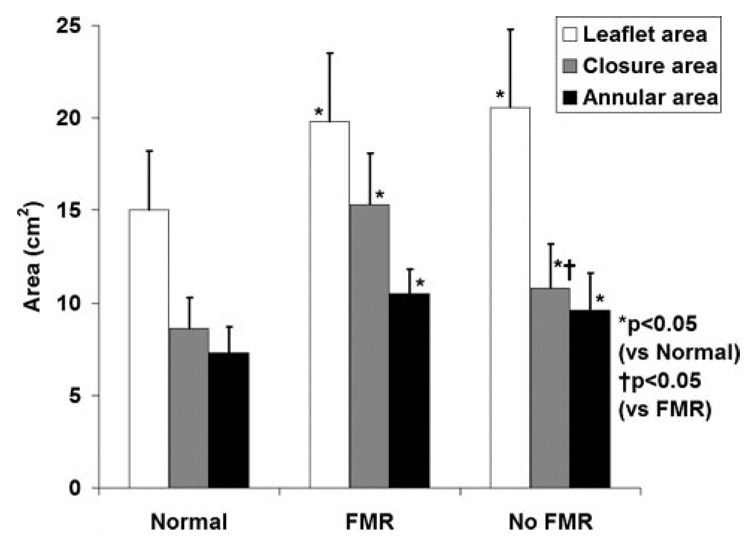
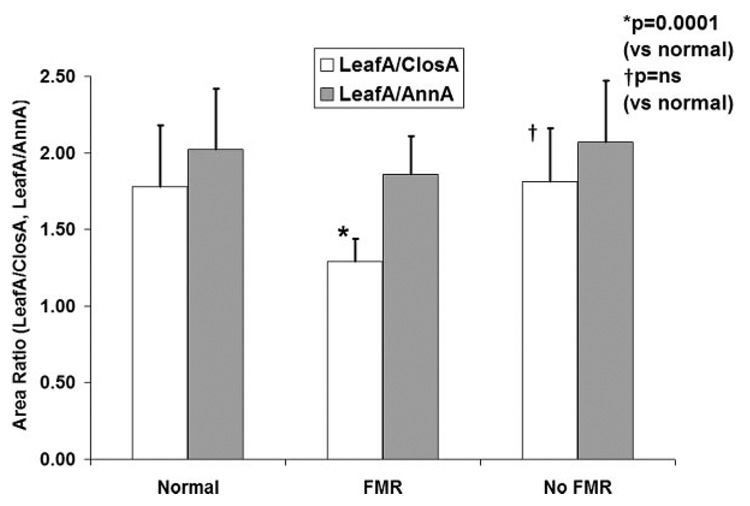
Methods and results: A new method for 3-dimensional echocardiographic measurement of mitral leaflet area was developed and validated in vivo against 15 sheep heart valves, later excised. This method was then applied in 80 consecutive patients from 3 groups: patients with normal hearts by echocardiography (n=20), patients with functional MR caused by isolated inferior wall-motion abnormality or dilated cardiomyopathy (n=29), and patients with inferior wall-motion abnormality or dilated cardiomyopathy but no MR (n=31). Leaflet area was increased by 35+/-20% in patients with LV dysfunction compared with normal subjects. The ratio of leaflet to annular area was 1.95+/-0.40 and was not different among groups, which indicates a surplus leaflet area that adapts to left-heart changes. In contrast, the ratio of total leaflet area to the area required to close the orifice in midsystole was decreased in patients with functional MR compared with those with normal hearts (1.29+/-0.15 versus 1.78+/-0.39, P=0.001) and compared with patients with inferior wall-motion abnormality or dilated cardiomyopathy but no MR (1.81+/-0.38, P=0.001). After adjustment for measures of LV remodeling and tethering, a leaflet-to-closure area ratio <1.7 was associated with significant MR (odds ratio 23.2, 95% confidence interval 2.0 to 49.1, P=0.02).
Conclusions: Mitral leaflet area increases in response to chronic tethering in patients with inferior wall-motion abnormality and dilated cardiomyopathy, but the development of significant MR is associated with insufficient leaflet area relative to that demanded by tethering geometry. The varying adequacy of leaflet adaptation may explain in part the heterogeneity of this disease among patients. The results suggest the need to understand the mechanisms that underlie leaflet adaptation and whether leaflet area can potentially be modified as part of the therapeutic approach.
Figures
Comment in
-
Is it time to update the definition of functional mitral regurgitation?: structural changes in the mitral leaflets with left ventricular dysfunction.Circulation. 2008 Aug 19;118(8):797-9. doi: 10.1161/CIRCULATIONAHA.108.795781. Circulation. 2008. PMID: 18711022 No abstract available.
References
-
- Grigioni F, Enriquez-Sarano M, Zehr KJ, Bailey KR, Tajik AJ. Ischemic mitral regurgitation: long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation. 2001;103:1759–1764. - PubMed
-
- Lamas GA, Mitchell GF, Flaker GC, Smith SC, Jr, Gersh BJ, Basta L, Moye L, Braunwald E, Pfeffer MA. Clinical significance of mitral regurgitation after acute myocardial infarction. Circulation. 1997;96:827–833. - PubMed
-
- Barzilai B, Gessler C, Perez JE, Schaab C, Jaffe AS. Significance of Doppler-detected mitral regurgitation in acute myocardial infarction. Am J Cardiol. 1988;61:220–223. - PubMed
-
- Feinberg MS, Schwammenthal E, Shlizerman L, Porter A, Hod H, Freimark D, Matezky S, Boyko V, Mandelzweig L, Vered Z. Prognostic significance of mild mitral regurgitation by color Doppler echocardiography in acute myocardial infarction. Am J Cardiol. 2000;86:903–907. - PubMed
-
- Ogawa S, Hubbard FE, Mardelli TJ, Dreifus LS. Cross-sectional echo-cardiographic spectrum of papillary muscle dysfunction. Am Heart J. 1979;97:312–321. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
