

Chemotherapy in addition to supportive care improves survival in advanced non-small-cell lung cancer: a systematic review and meta-analysis of individual patient data from 16 randomized controlled trials
- PMID: 18678835
- PMCID: PMC2653127
- DOI: 10.1200/JCO.2008.17.7162
Chemotherapy in addition to supportive care improves survival in advanced non-small-cell lung cancer: a systematic review and meta-analysis of individual patient data from 16 randomized controlled trials
Abstract
Purpose: Since our individual patient data (IPD) meta-analysis (MA) of supportive care and chemotherapy for non-small-cell lung cancer (NSCLC), published in 1995, many trials have been completed. An updated, IPD MA has been carried out to assess newer regimens and determine conclusively the effect of chemotherapy.
Methods: Systematic searches for randomized controlled trials (RCTs) were undertaken, followed by central collection, checking, and reanalysis of updated IPD. Results from RCTs were combined to calculate individual and pooled hazard ratios (HRs).
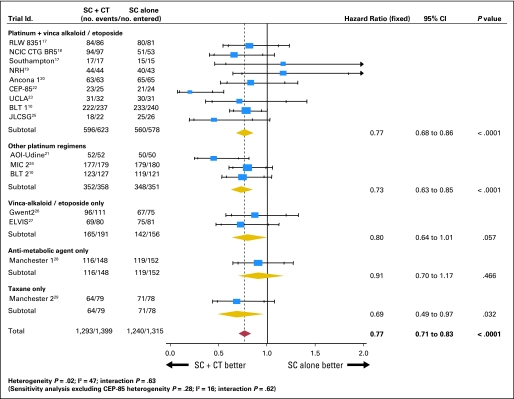
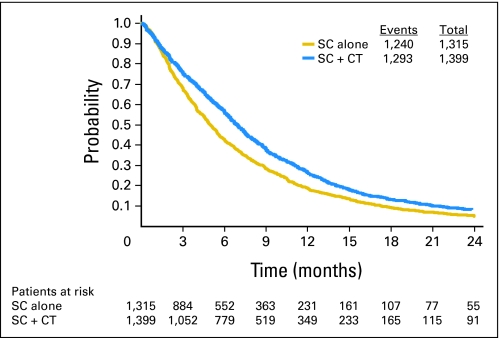
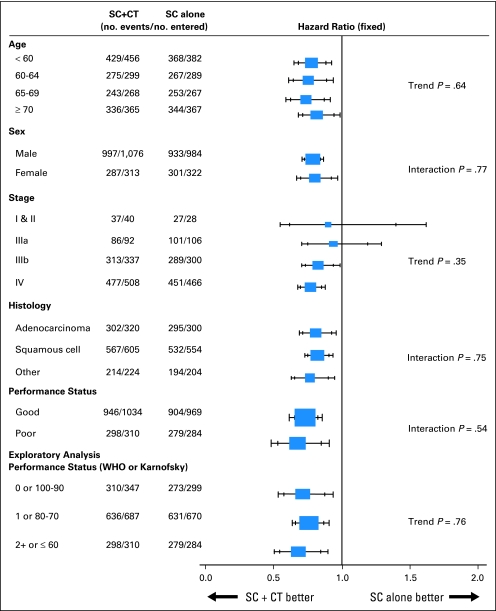
Results: Data were obtained from 2,714 patients from 16 RCTs. There were 1,293 deaths among 1,399 patients assigned supportive care and chemotherapy and 1,240 among 1,315 assigned supportive care alone. Results showed a significant benefit of chemotherapy (HR, 0.77; 95% CI, 0.71 to 0.83; P <or= .0001), equivalent to a relative increase in survival of 23% or an absolute improvement in survival of 9% at 12 months, increasing survival from 20% to 29%. There was no clear evidence that this effect was influenced by the drugs used (P = .63) or whether they were used as single agents or in combination (P = .40). Despite changes in patient demographics, the effect of chemotherapy in recent trials did not differ from those included previously (P = .77). There was no clear evidence of a difference or trend in the relative effect of chemotherapy across patient subgroups.
Conclusion: This MA of chemotherapy in the supportive care setting demonstrates conclusively that chemotherapy improves overall survival in all patients with advanced NSCLC. Therefore, all patients who are fit enough and wish to receive chemotherapy should do so.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, et al: Global cancer statistics, 2002. CA Cancer J Clin 55:74-108, 2005 - PubMed
-
- Visbal AL, Leighl NB, Feld R, et al: Adjuvant chemotherapy for early stage non-small cell lung cancer. Chest 128:2933-2943, 2005 - PubMed
-
- World Health Organization: Global cancer rates could increase by 50% to 15 million by 2020. http://www.who.int/mediacentre/news/releases/2003/pr27/en/
-
- Greenlee RT, Murray T, Bolden S, et al: Cancer Statistics, 2000. CA Cancer J Clin 50:7-33, 2000 - PubMed
-
- Rudd R: Chemotherapy in the treatment of non-small cell lung cancer. Respiratory Disease in Practice 7:12-14, 1991
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
