

Catheter ablation of fascicular ventricular tachycardia
- PMID: 18679520
- PMCID: PMC2490803
Catheter ablation of fascicular ventricular tachycardia
Abstract
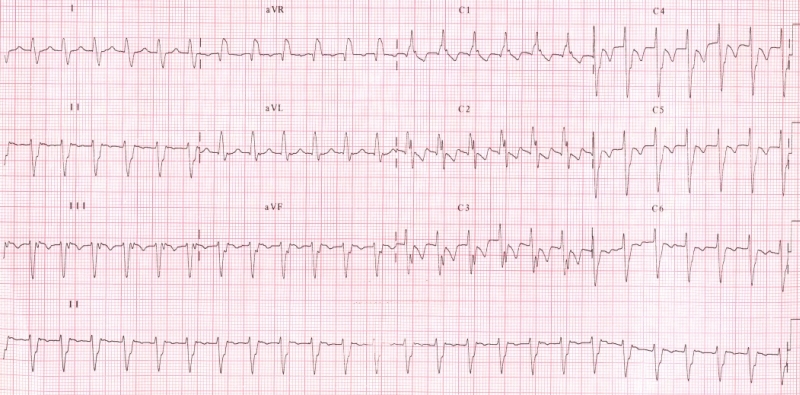
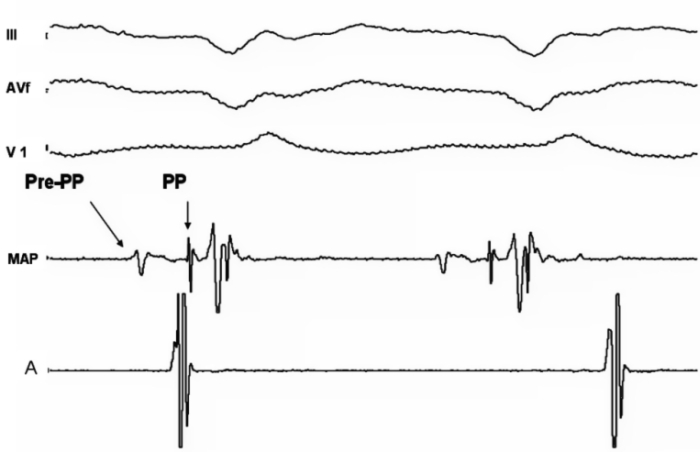
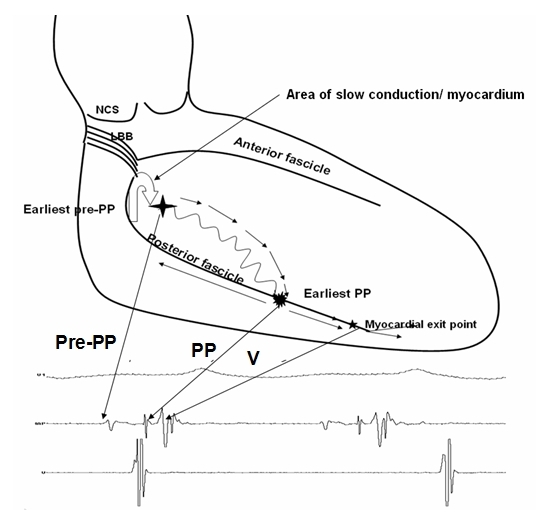
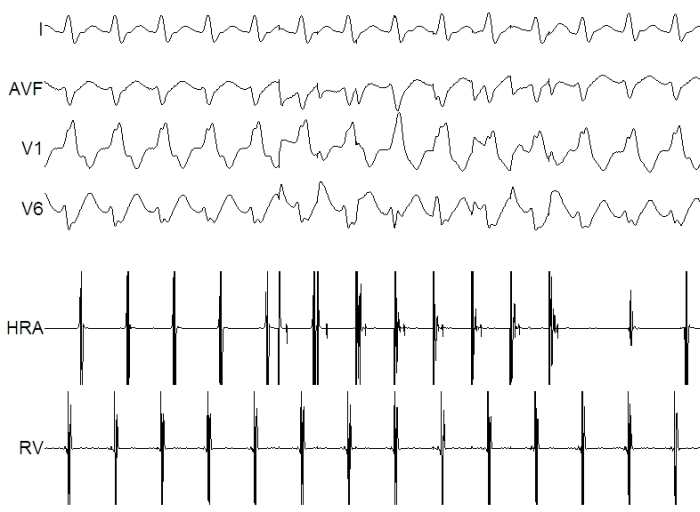
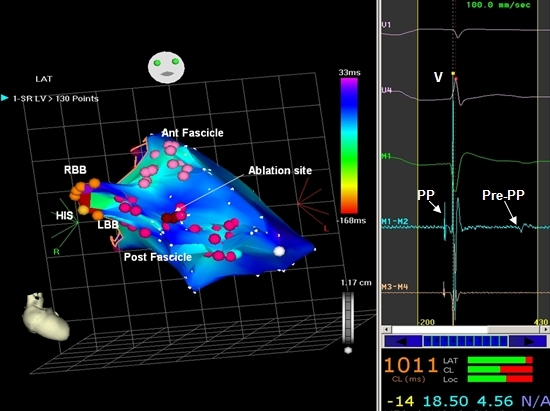
Fascicular ventricular tachycardia (VT) is an idiopathic VT with right bundle branch block morphology and left-axis deviation occuring predominantly in young males. Fascicular tachycardia has been classified into three subtypes namely, left posterior fascicular VT, left anterior fascicular VT and upper septal fascicular VT. The mechanism of this tachycardia is believed to be localized reentry close to the fascicle of the left bundle branch. The reentrant circuit is composed of a verapamil sensitive zone, activated antegradely during tachycardia and the fast conduction Purkinje fibers activated retrogradely during tachycardia recorded as the pre Purkinje and the Purkinje potentials respectively. Catheter ablation is the preferred choice of therapy in patients with fascicular VT. Ablation is carried out during tachycardia, using conventional mapping techniques in majority of the patients, while three dimensional mapping and sinus rhythm ablation is reserved for patients with nonmappable tachycardia.
Keywords: Fascicular ventricular tachycardia; Radiofrequency ablation.
Figures
References
-
- Zipes DP, Foster PR, Troup PJ, et al. Atrial induction of ventricular tachycardia: reentry versus triggered automaticity. Am J Cardiol. 1979;44:1–8. - PubMed
-
- Thakur RK, Klein GJ, Sivaram CA, et al. Anatomic substrate for idiopathic left ventricular tachycardia. Circulation. 1996;93:497–501. - PubMed
-
- Lin FC, Wen MS, Wang CC, et al. Left ventricular fibromuscular band is not a specific substrate for idiopathic left ventricular tachycardia. Circulation. 1996;93:525–528. - PubMed
LinkOut - more resources
Full Text Sources