

Rate of complications in scoliosis surgery - a systematic review of the Pub Med literature
- PMID: 18681956
- PMCID: PMC2525632
- DOI: 10.1186/1748-7161-3-9
Rate of complications in scoliosis surgery - a systematic review of the Pub Med literature
Abstract
Background: Spinal fusion surgery is currently recommended when curve magnitude exceeds 40-45 degrees. Early attempts at spinal fusion surgery which were aimed to leave the patients with a mild residual deformity, failed to meet such expectations. These aims have since been revised to the more modest goals of preventing progression, restoring 'acceptability' of the clinical deformity and reducing curvature.In view of the fact that there is no evidence that health related signs and symptoms of scoliosis can be altered by spinal fusion in the long-term, a clear medical indication for this treatment cannot be derived. Knowledge concerning the rate of complications of scoliosis surgery may enable us to establish a cost/benefit relation of this intervention and to improve the standard of the information and advice given to patients. It is also hoped that this study will help to answer questions in relation to the limiting choice between the risks of surgery and the "wait and see - observation only until surgery might be recommended", strategy widely used. The purpose of this review is to present the actual data available on the rate of complications in scoliosis surgery.
Materials and methods: Search strategy for identification of studies; Pub Med and the SOSORT scoliosis library, limited to English language and bibliographies of all reviewed articles. The search strategy included the terms; 'scoliosis'; 'rate of complications'; 'spine surgery'; 'scoliosis surgery'; 'spondylodesis'; 'spinal instrumentation' and 'spine fusion'.
Results: The electronic search carried out on the 1st February 2008 with the key words "scoliosis", "surgery", "complications" revealed 2590 titles, which not necessarily attributed to our quest for the term "rate of complications". 287 titles were found when the term "rate of complications" was used as a key word. Rates of complication varied between 0 and 89% depending on the aetiology of the entity investigated. Long-term rates of complications have not yet been reported upon.
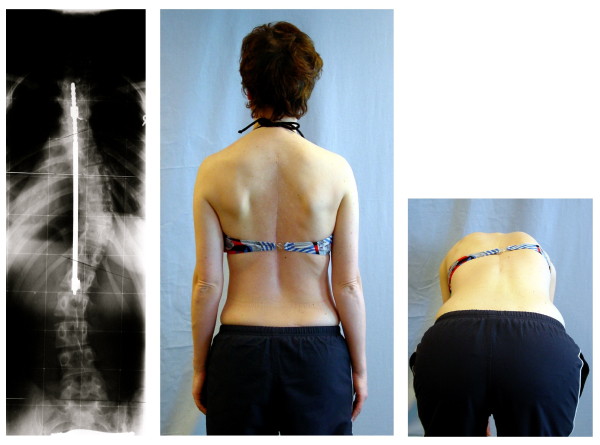
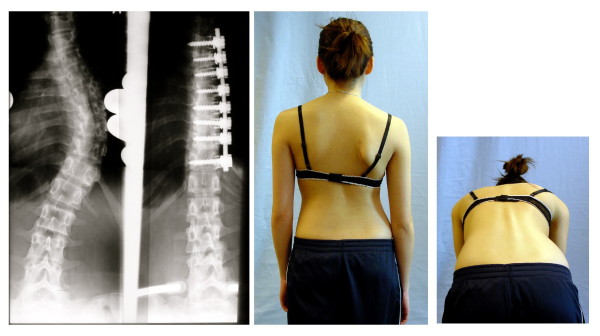
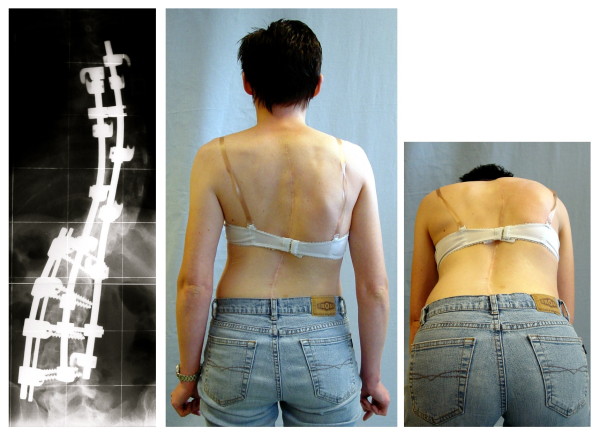
Conclusion: Scoliosis surgery has a varying but high rate of complications. A medical indication for this treatment cannot be established in view of the lack of evidence. The rate of complications may even be higher than reported. Long-term risks of scoliosis surgery have not yet been reported upon in research. Mandatory reporting for all spinal implants in a standardized way using a spreadsheet list of all recognised complications to reveal a 2-year, 5-year, 10-year and 20-year rate of complications should be established. Trials with untreated control groups in the field of scoliosis raise ethical issues, as the control group could be exposed to the risks of undergoing such surgery.
Figures

References
-
- Stokes IAF. Three dimensional terminology of spinal deformity: A report presented to the Scoliosis research Society by the Scoliosis Research Society Working Group on 3-D Terminology of Spinal Deformities. Spine. 1994;19:236–248. - PubMed
-
- Cobb JR. Outline for the study of scoliosis. In: Edwards JW, editor. AAOS, Instructional Course Lectures. Vol. 5. Ann Arbor: The American Academy of Orthopaedic Surgeons; 1948. pp. 261–75.
-
- Kleinberg S. The operative treatment of scoliosis. Arch Surg. 1922;5:631–645.
-
- Hawes MC. The use of exercises in the treatment of scoliosis: an evidence-based critical review of the literature. Pediatr Rehabil. 2003;6:171–82. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
