

Human papillomavirus 'reflex' testing as a screening method in cases of minor cytological abnormalities
- PMID: 18682715
- PMCID: PMC2527833
- DOI: 10.1038/sj.bjc.6604504
Human papillomavirus 'reflex' testing as a screening method in cases of minor cytological abnormalities
Abstract
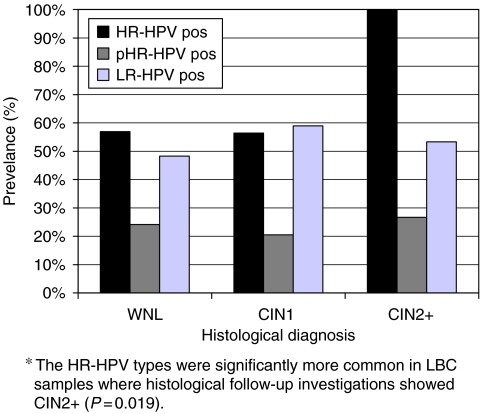
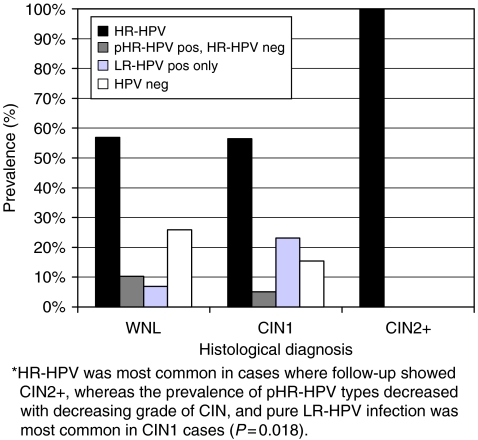
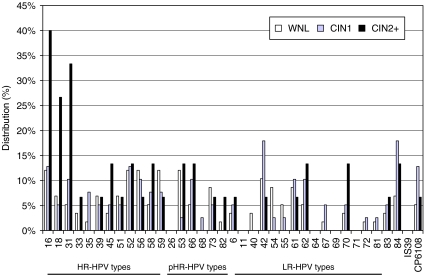
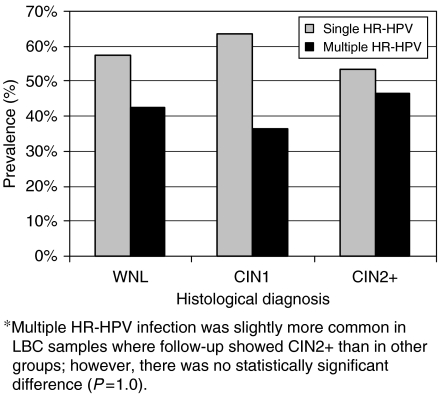
The aim was to evaluate human papillomavirus (HPV) 'reflex genotyping' in cases of minor cytological abnormalities detected in the gynaecological screening programme in Stockholm, Sweden. Liquid-based cytology samples showing minor cytological abnormalities were analysed using HPV genotyping (Linear Array, Roche diagnostics). Colposcopically directed cervical biopsies were obtained and the HPV test results were correlated with the histological results. In all, 63% (70/112) of the samples were high-risk (HR) HPV (HR-HPV) positive. A statistically significant correlation was found between high-grade cervical lesions and HR-HPV (P=0.019), among which HPV 16, 18, and 31 were the most important. The negative predictive value of HR-HPV detection for histologically confirmed high-grade lesions was 100%. An age limit for HPV reflex testing may be motivated in cases of low-grade squamous intraepithelial neoplasia (LSIL), because of high HR-HPV prevalence among younger women. By using HPV reflex genotyping, additional extensive workup can safely be avoided in about 50% of all cases of atypical squamous cells of undetermined significance (ASCUS) and LSIL among women 30 years. This screening strategy could potentially reduce the total abnormal cytology-reporting rate in the Swedish screening programme by about 1% and provide more accurately directed follow-up, guided by cytological appearance and HPV test results.
Figures
References
-
- Andersson S, Larson B, Hjerpe A, Silfverswärd C, Sällström J, Wilander E, Rylander E (2003) Adenocarcinoma of the uterine cervix: the presence of human papillomavirus and the method of detection. Acta Obstet Gynecol Scand 82: 960–965 - PubMed
-
- Andersson-Ellström A, Seidal T, Grannas M, Hagmar B (2000) The pap-smear history of women with invasive cervical squamous carcinoma. Acta Obstet Gynecol Scand 79: 221–226 - PubMed
-
- Andrae B, Kemetli L, Sparén P (2008) Screening-preventable cervical cancer risk: evidence for a nation-wide audit of cervical cancer in Sweden. J Nat Cancer Inst 100(9): 622–629 - PubMed
-
- Arbyn M, Sasieni P, Meijer CJ, Clavel C, Koliopoulos G, Dillner J (2006) Chapter 9: clinical applications of HPV testing: a summary of meta-analyses. Vaccine 24: 78–89 - PubMed
