

Analysis of nevirapine (NVP) resistance in Ugandan infants who were HIV infected despite receiving single-Dose (SD) NVP versus SD NVP plus daily NVP up to 6 weeks of age to prevent HIV vertical transmission
- PMID: 18684096
- PMCID: PMC2587235
- DOI: 10.1086/591503
Analysis of nevirapine (NVP) resistance in Ugandan infants who were HIV infected despite receiving single-Dose (SD) NVP versus SD NVP plus daily NVP up to 6 weeks of age to prevent HIV vertical transmission
Abstract
Background: Single-dose nevirapine (SD NVP) at birth plus NVP prophylaxis for the infant up to 6 weeks of age is superior to SD NVP alone for prevention of vertical transmission of human immunodeficiency virus (HIV) through breastfeeding. We analyzed NVP resistance in HIV-infected Ugandan infants who received either SD NVP or extended NVP prophylaxis.
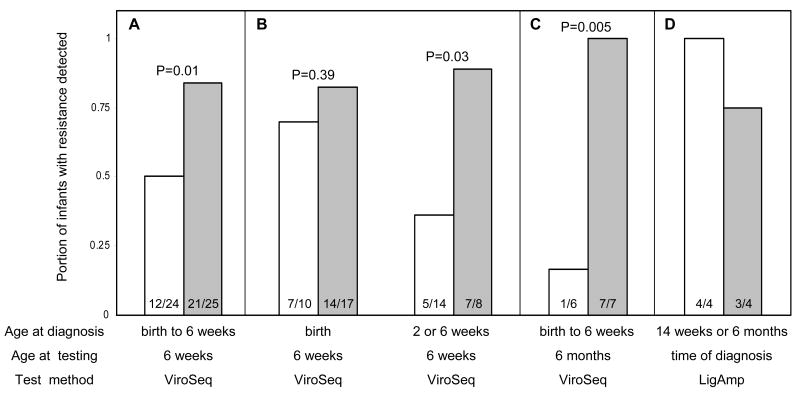
Methods: We tested plasma HIV by using a genotyping assay (ViroSeq; Celera Diagnostics), a phenotypic resistance assay (PhenoSense; Monogram Biosciences), and sensitive point mutation assay (LigAmp, for K103N, Y181C, and G190A).
Results: When infants were 6 weeks old, ViroSeq detected NVP resistance in a higher proportion of infants in the extended NVP arm than in the SD NVP arm (21 of 25 [84%] vs. 12 of 24 [50%]; P = .01). Similar results were obtained with LigAmp and PhenoSense. In both study arms, infants who were HIV infected at birth frequently had NVP resistance detected. In contrast, infants in the extended NVP arm who were HIV infected after birth were more likely to have resistance detected at 6 weeks, compared with infants in the SD NVP arm. The use of extended NVP prophylaxis was also associated with detection of NVP resistance by ViroSeq at 6 months (7 of 7 [100%] infants in the extended NVP arm had resistance detected, compared with 1 of 6 [16.7%] infants in the SD NVP arm; P = .005).
Conclusions: The use of extended NVP prophylaxis was associated with increased selection for and persistence of NVP resistance in HIV-infected Ugandan infants.
Conflict of interest statement
Figures
References
-
- Guay LA, Musoke P, Fleming T, et al. Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda: HIVNET 012 randomised trial. Lancet. 1999;354:795–802. - PubMed
-
- Jackson JB, Musoke P, Fleming T, et al. Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda: 18 months follow-up of the HIVNET 012 randomised trial. Lancet. 2003;362:859–868. - PubMed
-
- Eshleman SH, Mracna M, Guay LA, et al. Selection and fading of resistance mutations in women and infants receiving nevirapine to prevent HIV-1 vertical transmission (HIVNET 012) AIDS. 2001;15:1951–1957. - PubMed
-
- Eshleman SH, Hoover DR, Chen S, et al. Resistance after single dose nevirapine prophylaxis emerges in a high portion of Malawian newborns. AIDS. 2005;19:2167–2168. - PubMed
-
- Martinson NA, Morris L, Gray G, et al. Selection and persistence of viral resistance in HIV-infected children after exposure to single-dose nevirapine. J Acquir Immune Defic Syndr. 2006;44:148–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI068632/AI/NIAID NIH HHS/United States
- U01 AI048054/AI/NIAID NIH HHS/United States
- U01 AI038576/AI/NIAID NIH HHS/United States
- 5U01AI46745/AI/NIAID NIH HHS/United States
- R01 AI034235/AI/NIAID NIH HHS/United States
- 5U01AI038576-07/AI/NIAID NIH HHS/United States
- U01 AI046745/AI/NIAID NIH HHS/United States
- 1U01AI068613/AI/NIAID NIH HHS/United States
- 1U01AI068632/AI/NIAID NIH HHS/United States
- 3R01AI34235/AI/NIAID NIH HHS/United States
- 5U01AI48054/AI/NIAID NIH HHS/United States
- U01 AI068613/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
