

Extended-interval dosing of gentamicin for treatment of neonatal sepsis in developed and developing countries
- PMID: 18686550
- PMCID: PMC2740664
Extended-interval dosing of gentamicin for treatment of neonatal sepsis in developed and developing countries
Abstract
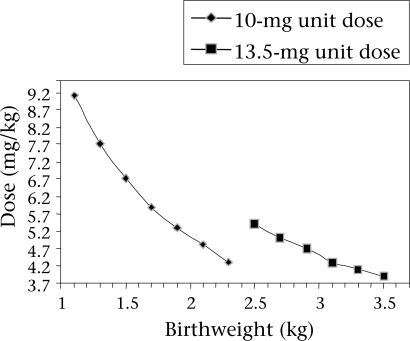
Serious bacterial infections are the single most important cause of neonatal mortality in developing countries. Case-fatality rates for neonatal sepsis in developing countries are high, partly because of inadequate administration of necessary antibiotics. For the treatment of neonatal sepsis in resource-poor, high-mortality settings in developing countries where most neonatal deaths occur, simplified treatment regimens are needed. Recommended therapy for neonatal sepsis includes gentamicin, a parenteral aminoglycoside antibiotic, which has excellent activity against gram-negative bacteria, in combination with an antimicrobial with potent gram-positive activity. Traditionally, gentamicin has been administered 2-3 times daily. However, recent evidence suggests that extended-interval (i.e. >24 hours) dosing may be applicable to neonates. This review examines the available data from randomized and non-randomized studies of extended-interval dosing of gentamicin in neonates from both developed and developing countries. Available data on the use of gentamicin among neonates suggest that extended dosing intervals and higher doses (>4 mg/kg) confer a favourable pharmacokinetic profile, the potential for enhanced clinical efficacy and decreased toxicity at reduced cost. In conclusion, the following simplified weight-based dosing regimen for the treatment of serious neonatal infections in developing countries is recommended: 13.5 mg (absolute dose) every 24 hours for neonates of >2,500 g, 10 mg every 24 hours for neonates of 2,000-2,499 g, and 10 mg every 48 hours for neonates of <2,000 g.
Figures
References
-
- Lawn JE, Cousens S, Zupan J. 4 million neonatal deaths: when? Where? Why? Lancet. 2005;365:891–900. - PubMed
-
- State of the world's newborns. Washington, DC: Save the Children Federation; 2001. Saving Newborn Lives; p. 28.
-
- Care of mother and baby at the health centre: a practical guide; report of a Technical Working Group, Geneva June 5-9, 1993. Geneva: World Health Organization; 1994. World Health Organization; pp. 11–2. (WHO/ FHE/MSM/94.2)
-
- Baqui AH, El Arifeen S, Seraji MHR, Mannan I, Rahman SM, Winch PJ, et al. Causes and timing of neonatal infectious morbidity and mortality in Sylhet district, Bangladesh: implications for programs (abstract) Pediatr Acad Soc. 2006;5555:295.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical