

Bisphosphonates in the management of postmenopausal osteoporosis--optimizing efficacy in clinical practice
- PMID: 18686751
- PMCID: PMC2546473
- DOI: 10.2147/cia.s2134
Bisphosphonates in the management of postmenopausal osteoporosis--optimizing efficacy in clinical practice
Abstract
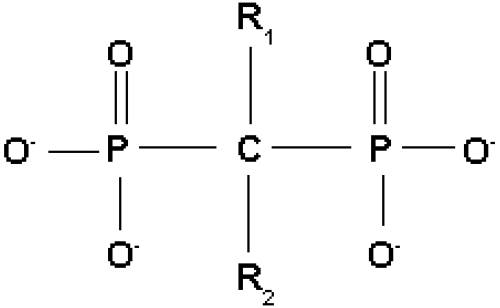
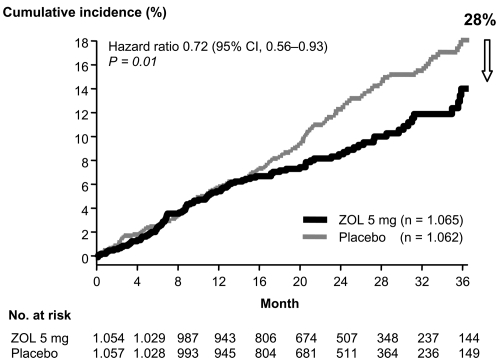
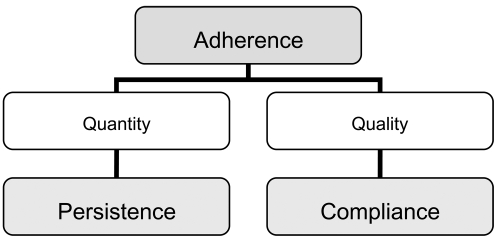
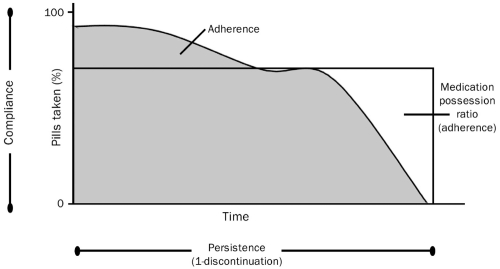
Nitrogen-containing bisphosphonates are potent inhibitors of osteoclastic bone resorption. With their individually proven efficacy to significantly reduce the incidence of vertebral and/or non-vertebral fractures and with their overall beneficial safety profile, alendronate, ibandronate, risedronate, and zoledronate are considered today a treatment of first choice in postmenopausal osteoporosis. However, treatment effects in an individual patient and cost-effectiveness in public health perspective are vitally dependent on the long-term patient adherence as well as on compliance and persistence. As compliance and persistence with daily oral bisphosphonates are shown to be suboptimal in many patients, leading to an increased fracture incidence in non-compliant patients, there is a need to improve overall adherence for bisphosphonate treatment in order to achieve maximum treatment effects. One option is to extend dosing intervals to weekly (alendronate, risedronate) or monthly (ibandronate) oral regimens. Less frequent oral regimens are generally preferred by majority of patients. Another alternative is intravenous, instead of oral application (ibandronate, zoledronate). Treatment acceptance could be further improved by IV bisphosphonates with their benefit of only quarterly, or even once-yearly, application. Treatment decisions should be based on anti-fracture efficacy data first. In addition, to ensure best possible patient adherence and maximum treatment benefits, physicians should consider individual patient conditions affecting compliance and persistence as well as patient preferences.
Conflict of interest statement
Figures
References
-
- Allen MR, Burr DB. Changes in vertebral strength-density and energy absorption-density relationships following bisphosphonate treatment in beagle dogs. Osteoporos Int. 2008;19:95–9. - PubMed
-
- Allen MR, Iwata K, Phipps R, et al. Risedronate and alendronate similarly suppress remodeling and increase microdamage in beagles after 1 year of treatment at clinical doses. J Bone Miner Res; 27th Annual Meeting of the American Society for Bone and Mineral Research 2005; Nashville, Tennessee, USA. 2005. p. S22.
-
- Badamgarav E, Fitzpatrick LA. A new look at osteoporosis outcomes: the influence of treatment, compliance, persistence, and adherence. Mayo Clin Proc. 2006;81:1009–12. - PubMed
-
- Baroutsou B, Babiolakis D, Stamatiadou A, et al. Patient compliance and preference of alendronate once weekly administration in comparison with daily regimens for osteoporotic postmenopausal women. Ann Rheum Dis. 2004;63(Suppl 1):455.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
