

A multivariate analysis of risk factors for the air-trapping asthmatic phenotype as measured by quantitative CT analysis
- PMID: 18689585
- PMCID: PMC2849984
- DOI: 10.1378/chest.08-0049
A multivariate analysis of risk factors for the air-trapping asthmatic phenotype as measured by quantitative CT analysis
Abstract
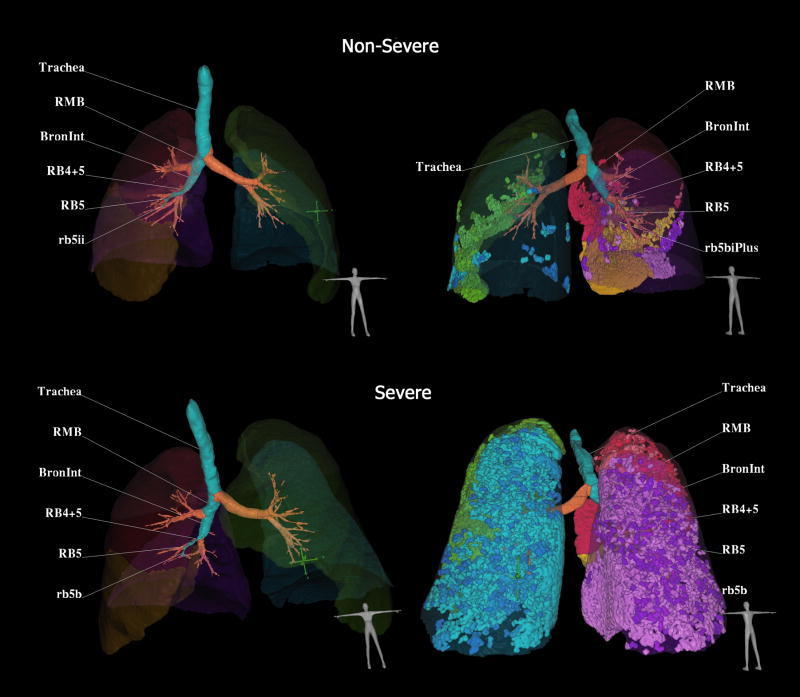
Background: Patients with severe asthma have increased physiologically measured air trapping; however, a study using CT measures of air trapping has not been performed. This study was designed to address two hypotheses: (1) air trapping measured by multidetector CT (MDCT) quantitative methodology would be a predictor of a more severe asthma phenotype; and (2) historical, clinical, allergic, or inflammatory risk factors could be identified via multivariate analysis.
Methods: MDCT scanning of a subset of Severe Asthma Research Program subjects was performed at functional residual capacity. Air trapping was defined as >or= 9.66% of the lung tissue < - 850 Hounsfield units (HU). Subjects classified as having air trapping were then compared to subjects without air trapping on clinical and demographic factors using both univariate and multivariate statistical analyses.
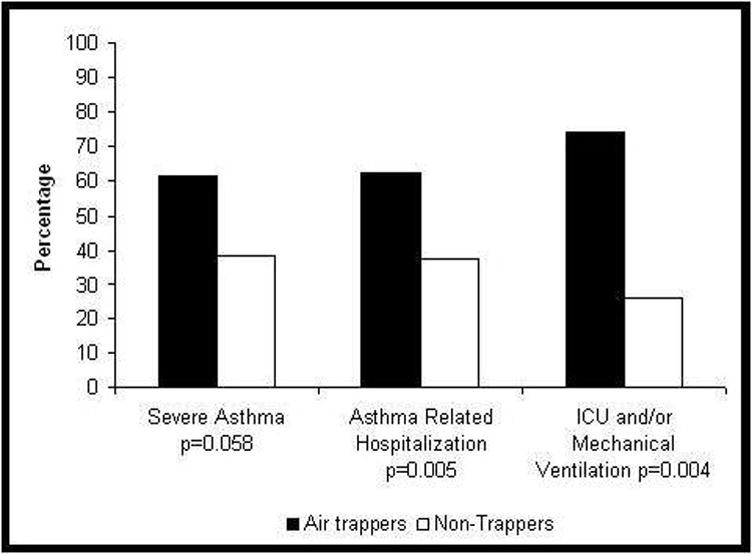
Results: Subjects with air trapping were significantly more likely to have a history of asthma-related hospitalizations, ICU visits, and/or mechanical ventilation. Duration of asthma (odds ratio [OR], 1.42; 95% confidence interval [CI], 1.08 to 1.87), history of pneumonia (OR, 8.55; 95% CI, 2.07 to 35.26), high levels of airway neutrophils (OR, 8.67; 95% CI, 2.05 to 36.57), airflow obstruction (FEV(1)/FVC) [OR, 1.61; 95% CI, 1.21 to 2.14], and atopy (OR, 11.54; 95% CI, 1.97 to 67.70) were identified as independent risk factors associated with the air-trapping phenotype.
Conclusions: Quantitative CT-determined air trapping in asthmatic subjects identifies a group of individuals at high risk for severe disease. Several independent risk factors for the presence of this phenotype were identified: perhaps most interestingly, history of pneumonia, neutrophilic inflammation, and atopy.
Conflict of interest statement
No authors have conflicts of interest to disclose.
Figures
References
-
- Wenzel S, Schwartz L, Langmack E, et al. Evidence that severe asthma can be divided pathologically into two inflammatory subtypes with distinct physiologic and clinical characteristics. Am J Respir Crit Care Med. 1999;160:1001–1008. - PubMed
-
- Coxson HO, Rogers RM, Whittall KP, et al. A Quantification of the Lung Surface Area in Emphysema Using Computed Tomography. Am J Respir Crit Care Med. 1999;159:851–856. - PubMed
-
- Madani A, Zanen J, de Maertelaer V, et al. Pulmonary emphysema: objective quantification at multi-detector row CT--comparison with macroscopic and microscopic morphometry. Radiology. 2006;238:1036–1043. - PubMed
-
- Jain N, Covar R, Gleason M, et al. Quantitative Computed Tomography Detects Peripheral Airway Disease in Asthmatic Children. Pediatr Pulmonol. 2005;40:211–218. - PubMed
Publication types
MeSH terms
Grants and funding
- HL69174/HL/NHLBI NIH HHS/United States
- R01 HL069155/HL/NHLBI NIH HHS/United States
- R01 HL069116/HL/NHLBI NIH HHS/United States
- HL-69155/HL/NHLBI NIH HHS/United States
- HL69349/HL/NHLBI NIH HHS/United States
- R01 HL069349/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- R01 HL069130/HL/NHLBI NIH HHS/United States
- HL69130/HL/NHLBI NIH HHS/United States
- R01 HL064368/HL/NHLBI NIH HHS/United States
- R01 HL069167/HL/NHLBI NIH HHS/United States
- HL69170/HL/NHLBI NIH HHS/United States
- HL69149/HL/NHLBI NIH HHS/United States
- HL69116/HL/NHLBI NIH HHS/United States
- R01 HL069174/HL/NHLBI NIH HHS/United States
- R01 HL069149/HL/NHLBI NIH HHS/United States
- R01 HL069170/HL/NHLBI NIH HHS/United States
- HL69167/HL/NHLBI NIH HHS/United States
- HL64368/HL/NHLBI NIH HHS/United States
- HL69174-05/HL/NHLBI NIH HHS/United States
- R01 HL059337/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
