

Agreement between patient-reported symptoms and their documentation in the medical record
- PMID: 18690769
- PMCID: PMC2581509
Agreement between patient-reported symptoms and their documentation in the medical record
Abstract
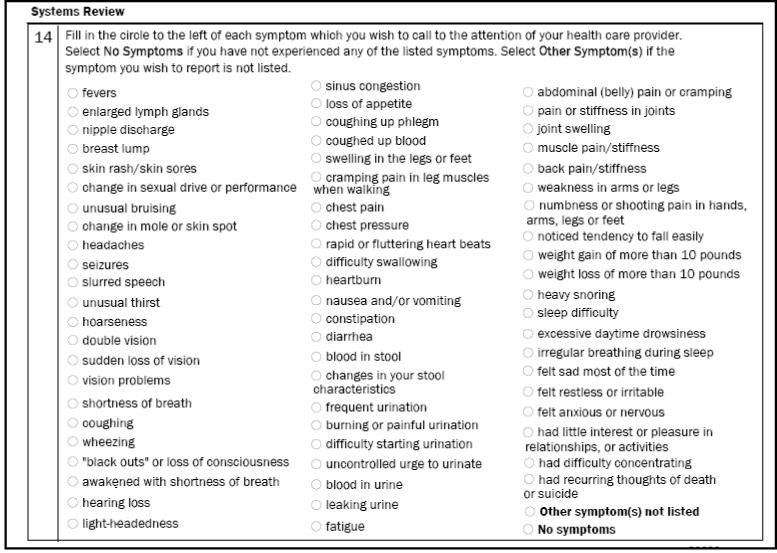
Objectives: To determine the agreement between patient-reported symptoms of chest pain, dyspnea, and cough and the documentation of these symptoms by physicians in the electronic medical record.
Methods: Symptoms reported on patient-provided information forms between January 1, 2006, and June 30, 2006, were compared with those identified by natural language processing of the text of clinical notes from care providers. Terms that represent the 3 symptoms were used to search clinical notes electronically with subsequent manual identification of the context (eg, affirmative, negated, family history) in which they occurred. Results were reported using positive and negative agreement, and kappa statistics.
Results: Symptoms reported by 1119 patients age 18 years or older were compared with the nonnegated terms identified in their clinical notes. Positive agreement was 74, 70, and 63 for chest pain, dyspnea, and cough, while negative agreement was 78, 76, and 75, respectively. Kappa statistics were 0.52 (95% confidence interval [CI] = 0.44, 0.60) for chest pain, 0.46 (95% CI = 0.37, 0.54) for dyspnea, and 0.38 (95% CI = 0.28, 0.48) for cough. Positive agreement was higher for older men (P >.05), and negative agreement was higher for younger women (P >.05).
Conclusions: We found discordance between patient self-report and documentation of symptoms in the medical record. This discordance has important implications for research studies that rely on symptom information for patient identification and may have clinical implications that must be evaluated for potential impact on quality of care, patient safety, and outcomes.
Figures


References
-
- Hing E, Cherry DK, Woodwell DA. National Ambulatory Medical Care Survey: 2004 summary. Adv Data. 2006;(374):1–33. - PubMed
-
- Lamberg L. New mind/body tactics target medically unexplained physical symptoms and fears. JAMA. 2005;294(17):2152–4. - PubMed
-
- Crossing the Quality Chasm: A New Health System for the 21st Century. Institute of Medicine; Washington, DC: 2001. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
