

A novel programme to evaluate and communicate 10-year risk of CHD reduces predicted risk and improves patients' modifiable risk factor profile
- PMID: 18691228
- PMCID: PMC2658032
- DOI: 10.1111/j.1742-1241.2008.01872.x
A novel programme to evaluate and communicate 10-year risk of CHD reduces predicted risk and improves patients' modifiable risk factor profile
Abstract
Aims: We assessed whether a novel programme to evaluate/communicate predicted coronary heart disease (CHD) risk could lower patients' predicted Framingham CHD risk vs. usual care.
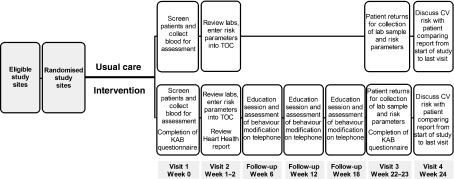
Methods: The Risk Evaluation and Communication Health Outcomes and Utilization Trial was a prospective, controlled, cluster-randomised trial in nine European countries, among patients at moderate cardiovascular risk. Following baseline assessments, physicians in the intervention group calculated patients' predicted CHD risk and were instructed to advise patients according to a risk evaluation/communication programme. Usual care physicians did not calculate patients' risk and provided usual care only. The primary end-point was Framingham 10-year CHD risk at 6 months with intervention vs. usual care.
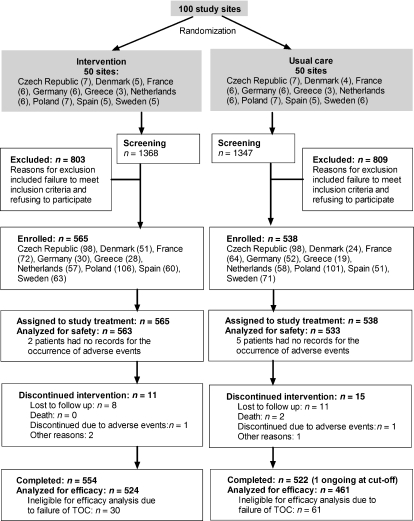
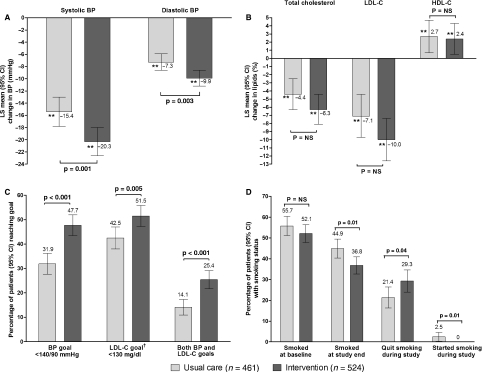
Results: Of 1103 patients across 100 sites, 524 patients receiving intervention, and 461 receiving usual care, were analysed for efficacy. After 6 months, mean predicted risks were 12.5% with intervention, and 13.7% with usual care [odds ratio = 0.896; p = 0.001, adjusted for risk at baseline (17.2% intervention; 16.9% usual care) and other covariates]. The proportion of patients achieving both blood pressure and low-density lipoprotein cholesterol targets was significantly higher with intervention (25.4%) than usual care (14.1%; p < 0.001), and 29.3% of smokers in the intervention group quit smoking vs. 21.4% of those receiving usual care (p = 0.04).
Conclusions: A physician-implemented CHD risk evaluation/communication programme improved patients' modifiable risk factor profile, and lowered predicted CHD risk compared with usual care. By combining this strategy with more intensive treatment to reduce residual modifiable risk, we believe that substantial improvements in cardiovascular disease prevention could be achieved in clinical practice.
Figures
References
-
- Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statistics – 2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–146. - PubMed
-
- Greenland P, Knoll MD, Stamler J, et al. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events. JAMA. 2003;290:891–7. - PubMed
-
- Neaton JD, Wentworth D. Serum cholesterol, blood pressure, cigarette smoking, and death from coronary heart disease. Overall findings and differences by age for 316,099 white men. Multiple Risk Factor Intervention Trial Research Group. Arch Intern Med. 1992;152:56–64. - PubMed
-
- Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–78. - PubMed
-
- Turnbull F, Neal B, Algert C, et al. Effects of different blood pressure-lowering regimens on major cardiovascular events in individuals with and without diabetes mellitus: results of prospectively designed overviews of randomized trials. Arch Intern Med. 2005;165:1410–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
