

Association between lower digit symbol substitution test score and slower gait and greater risk of mortality and of developing incident disability in well-functioning older adults
- PMID: 18691275
- PMCID: PMC2631090
- DOI: 10.1111/j.1532-5415.2008.01856.x
Association between lower digit symbol substitution test score and slower gait and greater risk of mortality and of developing incident disability in well-functioning older adults
Abstract
Objectives: To determine whether, in well-functioning older adults, a lower score on the Digit Symbol Substitution Test (DSST) and slower gait are associated with greater risk of mortality and of developing incident disability independent of other risk factors, including brain structural abnormalities (white matter hyperintensities, brain infarcts, ventricular enlargement) and whether the combination of varying levels of DSST score and gait speed are associated with a greater risk of mortality and disability than low DSST or slow gait alone.
Design: Observational cohort study.
Setting: Community.
Participants: Three thousand one hundred fifty-six (43% men, 29% black, mean age 70.4) participants in the Cardiovascular Health Study (CHS), free from stroke and physical disability and with a modified Mini-Mental State Examination (3MS) score of 80 or higher.
Measurements: Total mortality and incident disability (self-report of any difficulty performing one or more of the six activities of daily living) ascertained over a median follow-up time of 8.4 years.
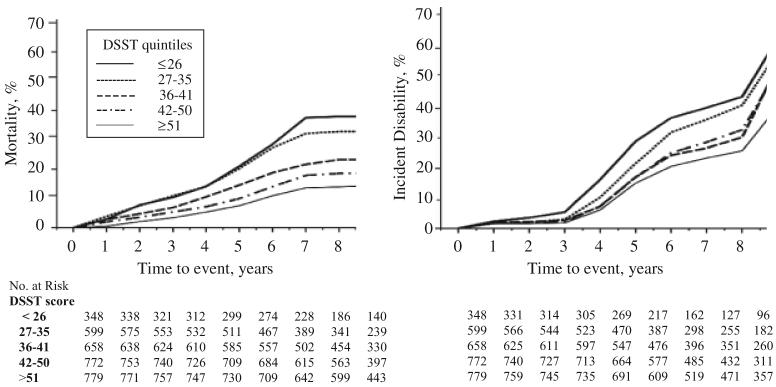
Results: By the end of follow-up, 704 participants had died and 1,096 had incident disability. In Cox proportional hazards models adjusted for age, sex, race, education, cardiovascular disease, and brain magnetic resonance imaging abnormalities, lower DSST score and slower gait remained significantly associated with greater risk of mortality and of incident disability. Mortality rates were higher in those who had both low DSST score (<27 points) and slow gait (speed <1.0 m/s) than in those who had only low DSST score, only slow gait, or neither (rates per 1,000 person years (p-y): 61.2, 42.8, 20.8, and 16.3, respectively). A similar risk gradient was observed for incident disability (82.0, 57.9, 47.9, and 36.0/1,000 p-y, respectively).
Conclusion: In well-functioning older adults, low DSST score and slow gait, alone or in combination, could be risk factors for mortality and for developing disability, independent of other risk factors, including measures of brain integrity.
Figures
Comment in
-
Visuospatial impairment and mortality.J Am Geriatr Soc. 2009 May;57(5):932-3. doi: 10.1111/j.1532-5415.2009.02247.x. J Am Geriatr Soc. 2009. PMID: 19470021 No abstract available.
Similar articles
-
Visuospatial impairment and mortality.J Am Geriatr Soc. 2009 May;57(5):932-3. doi: 10.1111/j.1532-5415.2009.02247.x. J Am Geriatr Soc. 2009. PMID: 19470021 No abstract available.
-
Subclinical brain magnetic resonance imaging abnormalities predict physical functional decline in high-functioning older adults.J Am Geriatr Soc. 2005 Apr;53(4):649-54. doi: 10.1111/j.1532-5415.2005.53214.x. J Am Geriatr Soc. 2005. PMID: 15817012
-
Digit Symbol Substitution test and future clinical and subclinical disorders of cognition, mobility and mood in older adults.Age Ageing. 2016 Sep;45(5):688-95. doi: 10.1093/ageing/afw116. Epub 2016 Jul 4. Age Ageing. 2016. PMID: 27496932 Free PMC article.
-
Long-term survival in adults 65 years and older with white matter hyperintensity: association with performance on the digit symbol substitution test.Psychosom Med. 2013 Sep;75(7):624-31. doi: 10.1097/PSY.0b013e31829c1df2. Epub 2013 Jul 25. Psychosom Med. 2013. PMID: 23886735 Free PMC article.
-
Is Low Psychomotor Speed a Marker of Brain Vulnerability in Late Life? Digit Symbol Substitution Test in the Prediction of Alzheimer, Parkinson, Stroke, Disability, and Depression.Dement Geriatr Cogn Disord. 2019;47(4-6):297-305. doi: 10.1159/000500597. Epub 2019 Aug 29. Dement Geriatr Cogn Disord. 2019. PMID: 31466055
Cited by
-
Putting the fear-avoidance model into practice - what can patients with chronic low back pain learn from patients with Achilles tendinopathy and vice versa?Braz J Phys Ther. 2023 Sep-Oct;27(5):100557. doi: 10.1016/j.bjpt.2023.100557. Epub 2023 Nov 4. Braz J Phys Ther. 2023. PMID: 37952338 Free PMC article.
-
Resting state connectivity within the basal ganglia and gait speed in older adults with cerebral small vessel disease and locomotor risk factors.Neuroimage Clin. 2020;28:102401. doi: 10.1016/j.nicl.2020.102401. Epub 2020 Aug 28. Neuroimage Clin. 2020. PMID: 32932053 Free PMC article.
-
Inflammation Mediates Body Weight and Ageing Effects on Psychomotor Slowing.Sci Rep. 2019 Oct 31;9(1):15727. doi: 10.1038/s41598-019-52062-3. Sci Rep. 2019. PMID: 31673089 Free PMC article.
-
Determinants of gait speed in COPD.Chest. 2014 Jul;146(1):104-110. doi: 10.1378/chest.13-2017. Chest. 2014. PMID: 24522522 Free PMC article.
-
Assessment in Work Productivity and the Relationship with Cognitive Symptoms (AtWoRC): primary analysis from a Canadian open-label study of vortioxetine in patients with major depressive disorder (MDD).CNS Spectr. 2019 Jun;24(3):338-347. doi: 10.1017/S1092852918000913. Epub 2018 May 24. CNS Spectr. 2019. PMID: 29792585 Free PMC article. Clinical Trial.
References
-
- Pavlik VN, de Moraes SA, Szklo M, et al. Relation between cognitive function and mortality in middle-aged adults: The Atherosclerosis Risk in Communities Study. Am J Epidemiol. 2003;157:327–334. - PubMed
-
- Royall DR, Chiodo L, Polk M. An empiric approach to level of care determinations: The importance of executive measures. J Gerontol A Biol Sci Med Sci. 2005;60A:1059–1064. - PubMed
-
- Royall DR, Palmer R, Chiodo L, et al. Declining executive control in normal aging predicts change in functional status: The Freedom House Study. J Am Geriatr Soc. 2004;52:346–352. - PubMed
-
- Schupf N, Tang MX, Albert SM, et al. Decline in cognitive and functional skills increases mortality risk in nondemented elderly. Neurology. 2005;65:1218–1226. - PubMed
-
- Dewey ME, Saz P. Dementia, cognitive impairment and mortality in persons aged 65 and over living in the community: A systematic review of the literature. Int J Geriatr Psychiatry. 2001;16:751–761. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
