

Temporary sutureless amniotic membrane patch for acute alkaline burns
- PMID: 18695099
- PMCID: PMC2849136
- DOI: 10.1001/archopht.126.8.1059
Temporary sutureless amniotic membrane patch for acute alkaline burns
Abstract
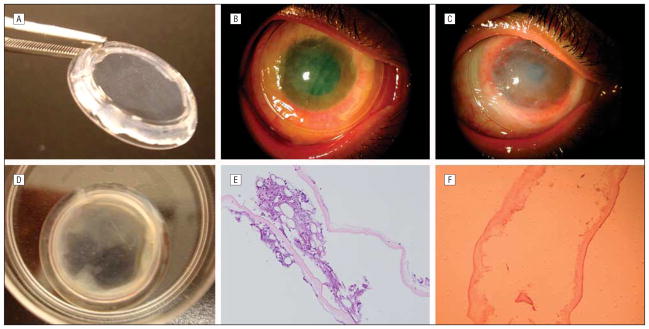
Objective: To evaluate the clinical outcome of a new sutureless approach for a temporary amniotic membrane patch (ProKera; Bio-Tissue, Inc, Miami, Florida) in eyes with acute burns.
Methods: Retrospective review of 5 eyes of 5 patients with grades I to III acute alkaline burns, receiving ProKera insertion within 8 days of injury.
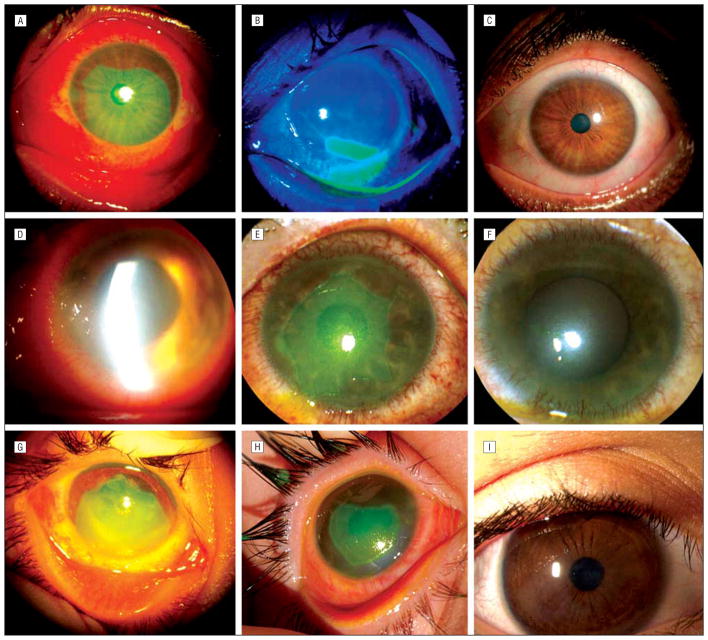
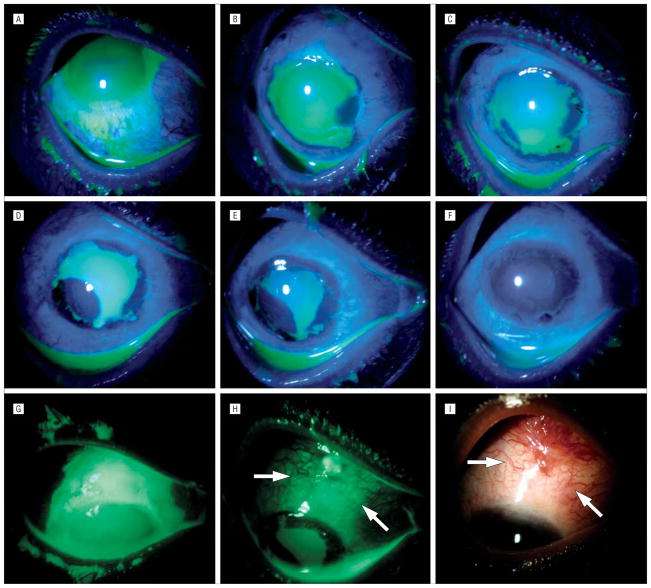
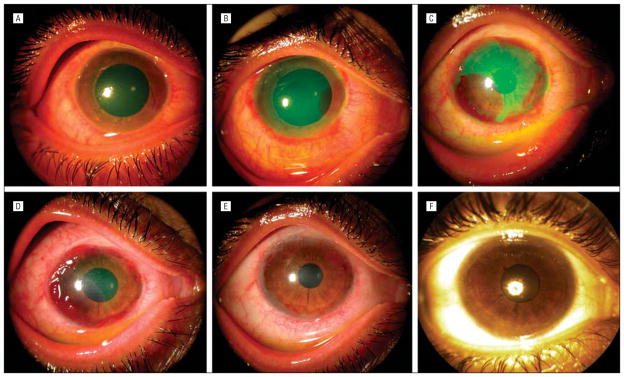
Results: These eyes had either total (2 cases) or extensive (60%-75%, 3 cases) corneal epithelial defects with limbal (120 degrees -360 degrees ) and conjunctival (30%-60%) epithelial defects. ProKera was inserted within a mean (SD) of 3.7 (3.1) days after burn and repeated 1 to 3 times for 3 cases. Conjunctival defects reepithelialized in 8.2 (5) days (range, 5-17 days), while limbal and corneal defects healed in 13.6 (8.3) days (range, 5-25 days). The latter was completed with circumferential closure of limbal defects followed by centripetal healing of corneal defects. In 3 eyes, early peripheral corneal neovascularization was followed by marked regression on completion of healing. During 16.8 (10.8) months of follow-up, all eyes retained a stable surface with improved corneal clarity, and without limbal deficiency or symblepharon.
Conclusion: This sutureless application of an amniotic membrane patch allows for early delivery of its biologic actions, which may help preserve remaining limbal stem cells for rapid expansion and prevent late cicatricial complications in eyes with mild and moderate acute alkaline burns.
Figures
References
-
- Wagoner MD. Chemical injuries of the eye: current concepts in pathophysiology and therapy. Surv Ophthalmol. 1997;41(4):275–313. - PubMed
-
- Levinson RA, Paterson CA, Pfister RR. Ascorbic acid prevents corneal ulceration and perforation following experimental alkali burns. Invest Ophthalmol Vis Sci. 1976;15(12):986–993. - PubMed
-
- Pfister RR, Nicolaro ML, Paterson CA. Sodium citrate reduces the incidence of corneal ulcerations and perforations in extreme alkali-burned eyes—acetylcysteine and ascorbate have no favorable effect. Invest Ophthalmol Vis Sci. 1981;21(3):486–490. - PubMed
-
- Seedor JA, Perry HD, McNamara TF, et al. Systemic tetracycline treatment of alkali-induced corneal ulceration in rabbits. Arch Ophthalmol. 1987;105(2):268–271. - PubMed
-
- Newsome NA, Gross J. Prevention by medroxyprogesterone of perforation in the alkali-burned rabbit cornea: inhibition of collagenolytic activity. Invest Ophthalmol Vis Sci. 1977;16(1):21–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
