

Radical prostatectomy versus watchful waiting in localized prostate cancer: the Scandinavian prostate cancer group-4 randomized trial
- PMID: 18695132
- PMCID: PMC2518167
- DOI: 10.1093/jnci/djn255
Radical prostatectomy versus watchful waiting in localized prostate cancer: the Scandinavian prostate cancer group-4 randomized trial
Abstract
Background: The benefit of radical prostatectomy in patients with early prostate cancer has been assessed in only one randomized trial. In 2005, we reported that radical prostatectomy improved prostate cancer survival compared with watchful waiting after a median of 8.2 years of follow-up. We now report results after 3 more years of follow-up.
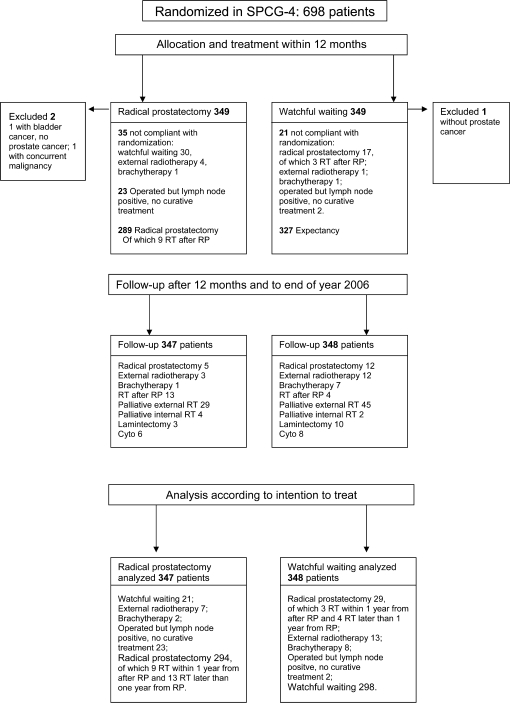
Methods: From October 1, 1989, through February 28, 1999, 695 men with clinically localized prostate cancer were randomly assigned to radical prostatectomy (n = 347) or watchful waiting (n = 348). Follow-up was complete through December 31, 2006, with histopathologic review and blinded evaluation of causes of death. Relative risks (RRs) were estimated using the Cox proportional hazards model. Statistical tests were two-sided.
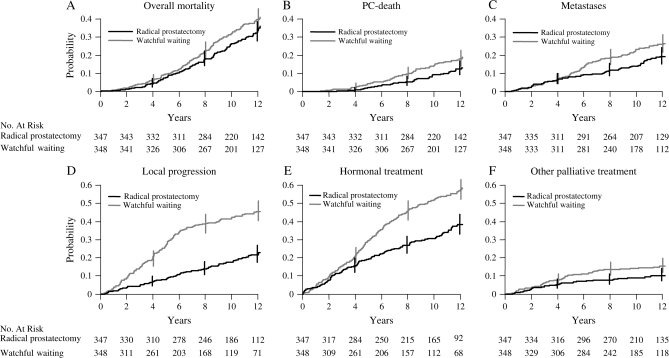
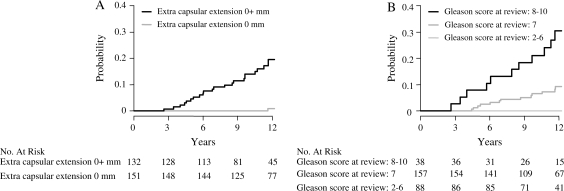
Results: During a median of 10.8 years of follow-up (range = 3 weeks to 17.2 years), 137 men in the surgery group and 156 in the watchful waiting group died (P = .09). For 47 of the 347 men (13.5%) who were randomly assigned to surgery and 68 of the 348 men (19.5%) who were not, death was due to prostate cancer. The difference in cumulative incidence of death due to prostate cancer remained stable after about 10 years of follow-up. At 12 years, 12.5% of the surgery group and 17.9% of the watchful waiting group had died of prostate cancer (difference = 5.4%, 95% confidence interval [CI] = 0.2 to 11.1%), for a relative risk of 0.65 (95% CI = 0.45 to 0.94; P = .03). The difference in cumulative incidence of distant metastases did not increase beyond 10 years of follow-up. At 12 years, 19.3% of men in the surgery group and 26% of men in the watchful waiting group had been diagnosed with distant metastases (difference = 6.7%, 95% CI = 0.2 to 13.2%), for a relative risk of 0.65 (95% CI = 0.47 to 0.88; P = .006). Among men who underwent radical prostatectomy, those with extracapsular tumor growth had 14 times the risk of prostate cancer death as those without it (RR = 14.2, 95% CI = 3.3 to 61.8; P < .001).
Conclusion: Radical prostatectomy reduces prostate cancer mortality and risk of metastases with little or no further increase in benefit 10 or more years after surgery.
Figures
Comment in
-
SPCG-4: a needed START to PIVOTal data to promote and protect evidence-based prostate cancer care.J Natl Cancer Inst. 2008 Aug 20;100(16):1123-5. doi: 10.1093/jnci/djn259. Epub 2008 Aug 11. J Natl Cancer Inst. 2008. PMID: 18695131 No abstract available.
-
A challenge to contemporary management of prostate cancer.Nat Clin Pract Urol. 2009 Jan;6(1):12-3. doi: 10.1038/ncpuro1270. Epub 2008 Dec 9. Nat Clin Pract Urol. 2009. PMID: 19065140
-
Re: Prostatectomy versus watchful waiting in localized prostate cancer: the Scandinavian Prostate Cancer Group-4 randomized trial.J Natl Cancer Inst. 2009 Jan 21;101(2):124. doi: 10.1093/jnci/djn443. Epub 2009 Jan 13. J Natl Cancer Inst. 2009. PMID: 19141784 No abstract available.
-
Words of wisdom. Re: Radical prostatectomy versus watchful waiting in localized prostate cancer: the Scandinavian Prostate Cancer Group-4 randomized trial.Eur Urol. 2009 Apr;55(4):989-90. doi: 10.1016/j.eururo.2009.01.009. Eur Urol. 2009. PMID: 19650212 No abstract available.
References
-
- Kvåle R, Auvinen A, Adami HO, et al. Interpreting trends in prostate cancer incidence and mortality in the five Nordic countries. J Natl Cancer Inst. 2007;99(24):1881–1887. - PubMed
-
- Adami HO, Baron JA, Rothman KJ. Ethics of a prostate cancer screening trial. Lancet. 1994;343(8903):958–960. - PubMed
-
- Draisma G, Boer R, Otto SJ, et al. Lead times and overdetection due to prostate-specific antigen screening: estimates from the European Randomized Study of Screening for Prostate Cancer. J Natl Cancer Inst. 2003;95(12):868–878. - PubMed
-
- Bill-Axelson A, Holmberg L, Ruutu M, et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2005;352(19):1977–1984. - PubMed
-
- Holmberg L, Bill-Axelson A, Helgesen F, et al. A randomized trial comparing radical prostatectomy with watchful waiting in early prostate cancer. N Engl J Med. 2002;347(11):781–799. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
