

Insulin resistance postburn: underlying mechanisms and current therapeutic strategies
- PMID: 18695610
- PMCID: PMC3905460
- DOI: 10.1097/BCR.0b013e31818481ce
Insulin resistance postburn: underlying mechanisms and current therapeutic strategies
Abstract
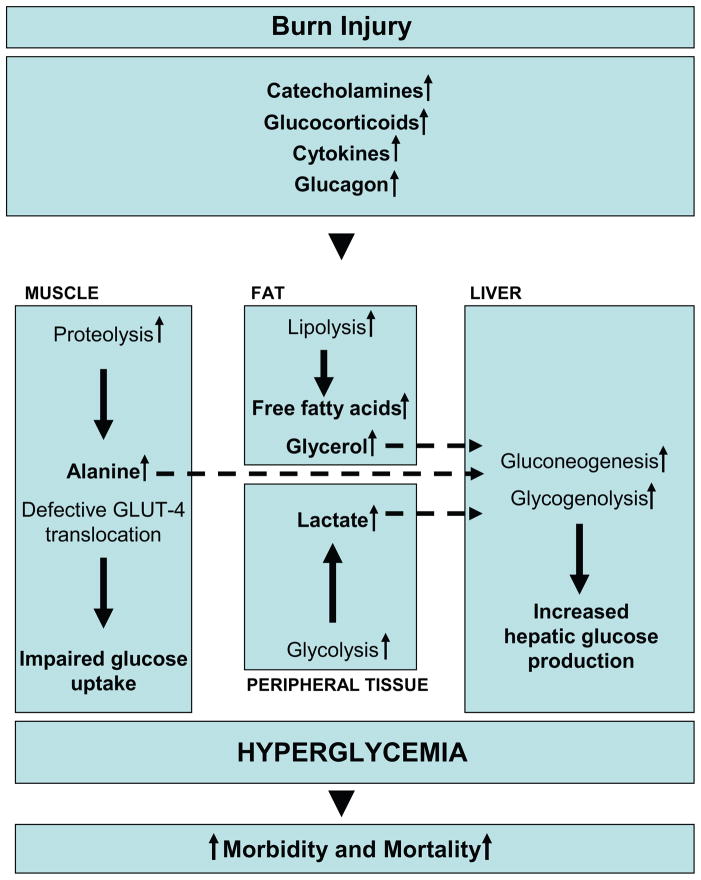
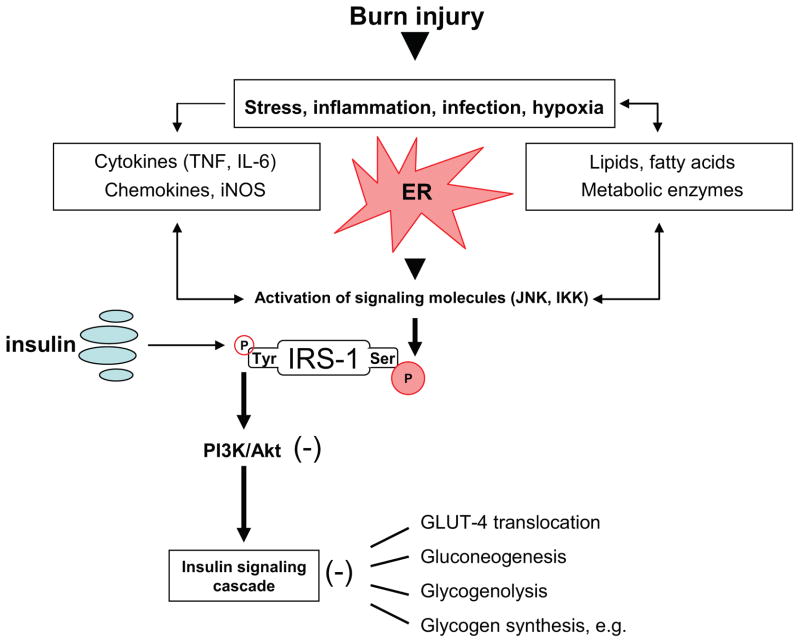
The profound hypermetabolic response to burn injury is associated with insulin resistance and hyperglycemia, significantly contributing to the incidence of morbidity and mortality in this patient population. These responses are present in all trauma, surgical, or critically ill patients, but the severity, length, and magnitude is unique for burn patients. Although advances in therapeutic strategies to attenuate the postburn hypermetabolic response have significantly improved the clinical outcome of these patients during the past years, therapeutic approaches to overcome stress-induced hyperglycemia have remained challenging. Intensive insulin therapy has been shown to significantly reduce morbidity and mortality in critically ill patients. High incidence of hypoglycemic events and difficult blood glucose titrations have led to investigation of alternative strategies, including the use of metformin, a biguanide, or fenofibrate, a peroxisome proliferator-activated receptor (PPAR)-gamma agonist. Nevertheless, weaknesses and potential side affects of these drugs reinforces the need for better understanding of the molecular mechanisms underlying insulin resistance postburn that may lead to novel therapeutic strategies further improving the prognosis of these patients. This review aims to discuss the mechanisms underlying insulin resistance induced hyperglycemia postburn and outlines current therapeutic strategies that are being used to modulate hyperglycemia after thermal trauma.
Figures
References
-
- Guidelines for the operation of burn centers. J Burn Care Res. 2007;28:134–41. - PubMed
-
- Brigham PA, McLoughlin E. Burn incidence and medical care use in the United States: estimates, trends, and data sources. J Burn Care Rehabil. 1996;17:95–107. - PubMed
-
- Wolf SE. Critical care in the severely burned: organ support and management of complications. In: Herndon DN, editor. Total Burn Care. 3. London: Saunders Elsevier; 2007. pp. 454–76.
-
- Herndon DN. Total Burn Care. 3. Philadelphia: Saunders Elsevier; 2007.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
