

Insulin protein and proliferation in ductal cells in the transplanted pancreas of patients with type 1 diabetes and recurrence of autoimmunity
- PMID: 18696047
- PMCID: PMC3019613
- DOI: 10.1007/s00125-008-1105-x
Insulin protein and proliferation in ductal cells in the transplanted pancreas of patients with type 1 diabetes and recurrence of autoimmunity
Abstract
Aim/hypothesis: We investigated whether beta cell neoformation occurs in the transplanted pancreas in patients with type 1 diabetes who had received a simultaneous pancreas-kidney transplant (SPK) and later developed recurrence of autoimmunity.
Methods: We examined pancreas transplant biopsies from nine SPK patients with or without recurrent autoimmunity or recurrent diabetes and from 16 non-diabetic organ donors. Tissues were analysed by immunohistochemistry and immunofluorescence.
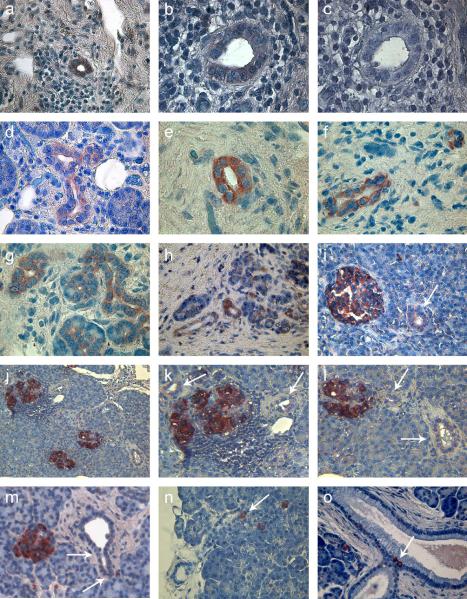
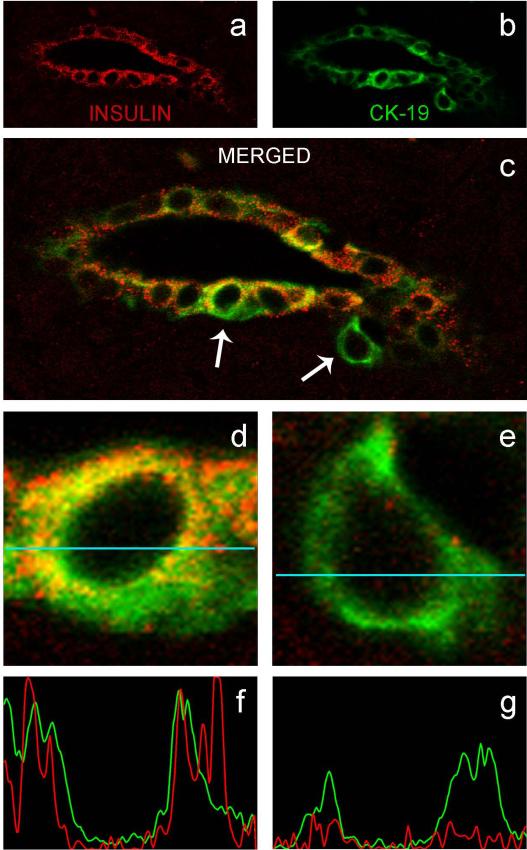
Results: Numerous cytokeratin-19 (CK-19)(+) pancreatic ductal cells stained for insulin in six SPK recipients with recurrent autoimmunity, in five of whom diabetes requiring insulin therapy recurred. These cells also stained for the transcription factor pancreatic-duodenal homeobox-1 (Pdx-1), which is implicated in pancreatic development and beta cell differentiation. The number of insulin(+) ductal cells varied, being highest in the patient with the most severe beta cell loss and lowest in the normoglycaemic patient. In the patient with the most severe beta cell loss, we detected insulin(+)CK-19(+)Pdx-1(+) cells staining for the proliferation-related Ki-67 antigen (Ki-67), indicating proliferation. We were unable to detect Ki-67(+) beta cells within the islets in any SPK patient. Some insulin(+)CK-19(-) ductal cells contained chromogranin A, suggesting further endocrine differentiation. Insulin(+) cells were rarely noted in the pancreas transplant ducts in three SPK patients without islet autoimmunity and in six of 16 non-diabetic organ donors; these insulin(+) cells were never CK-19(+).
Conclusions/interpretation: Insulin(+) pancreatic ductal cells, some apparently proliferating, were found in the transplanted pancreas with recurrent islet autoimmunity/diabetes. Replicating beta cells were not detected within islets. The observed changes may represent attempts at tissue remodelling and beta cell regeneration involving ductal cells in the human transplanted pancreas, possibly stimulated by hyperglycaemia and chronic inflammation.
Figures



References
-
- Tsai EB, Sherry NA, Palmer JP, Herold KC. The rise and fall of insulin secretion in type 1 diabetes mellitus. Diabetologia. 2006;49:261–270. - PubMed
-
- Gepts W, De Mey J. Islet cell survival determined by morphology. An immunocytochemical study of the islets of Langerhans in juvenile diabetes mellitus. Diabetes. 1978;27:251–261. - PubMed
-
- Rahier J, Goebbels RM, Henquin JC. Cellular composition of the human diabetic pancreas. Diabetologia. 1983;24:366–371. - PubMed
-
- Lohr M, Kloppel G. Residual insulin positivity and pancreatic atrophy in relation to duration of chronic type 1 (insulin-dependent) diabetes mellitus and microangiopathy. Diabetologia. 1987;30:757–762. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
