

An improved algorithm for femoropopliteal artery centerline restoration using prior knowledge of shapes and image space data
- PMID: 18697561
- PMCID: PMC2673553
- DOI: 10.1118/1.2940194
An improved algorithm for femoropopliteal artery centerline restoration using prior knowledge of shapes and image space data
Abstract
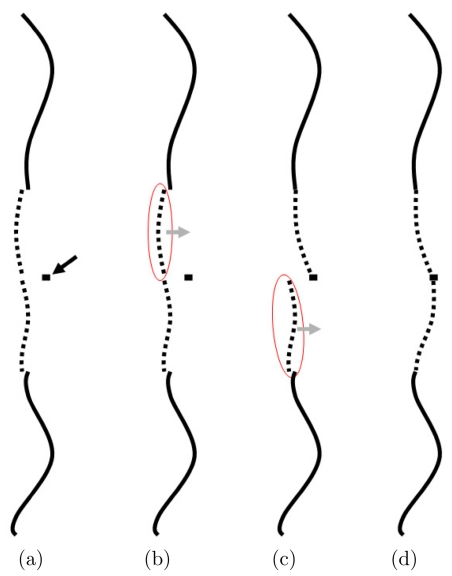
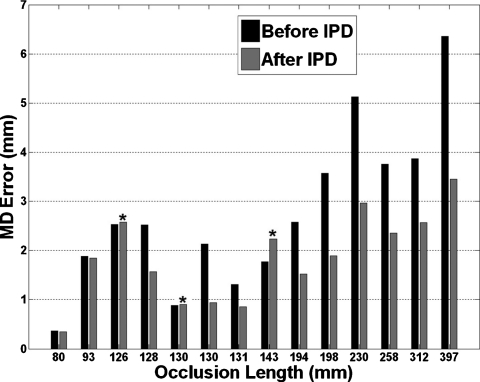
Accurate arterial centerline extraction is essential for comprehensive visualization in CT Angiography. Time consuming manual tracking is needed when automated methods fail to track centerlines through severely diseased and occluded vessels. A previously described algorithm, Partial Vector Space Projection (PVSP), which uses vessel shape information from a database to bridge occlusions of the femoropopliteal artery, has a limited accuracy in long (>100 mm) occlusions. In this article we introduce a new algorithm, Intermediate Point Detection (IPD), which uses calcifications in the occluded artery to provide additional information about the location of the centerline to facilitate improvement in PVSP performance. It identifies calcified plaque in image space to find the most useful point within the occlusion to improve the estimate from PVSP. In this algorithm candidates for calcified plaque are automatically identified on axial CT slices in a restricted region around the estimate obtained from PVSP. A modified Canny edge detector identifies the edge of the calcified plaque and a convex polygon fit is used to find the edge of the calcification bordering the wall of the vessel. The Hough transform for circles estimates the center of the vessel on the slice, which serves as a candidate intermediate point. Each candidate is characterized by two scores based on radius and relative position within the occluded segment, and a polynomial function is constructed to define a net score representing the potential benefit of using this candidate for improving the centerline. We tested our approach in 44 femoropopliteal artery occlusions of lengths up to 398 mm in 30 patients with peripheral arterial occlusive disease. Centerlines were tracked manually by four-experts, twice each, with their mean serving as the reference standard. All occlusions were first interpolated with PVSP using a database of femoropopliteal arterial shapes obtained from a total of 60 subjects. Occlusions longer than 80 mm (N = 20) were then processed with the IPD algorithm, provided calcifications were found (N = 14). We used the maximum point-wise distance of an interpolated curve from the reference standard as our error metric. The IPD algorithm significantly reduced the average error of the initial PVSP from 2.76 to 1.86 mm (p < 0.01). The error was less than the clinically desirable 3 mm (smallest radius of the femoropopliteal artery) in 13 of 14 occlusions. The IPD algorithm achieved results within the range of the human readers in 11 of 14 cases. We conclude that the additional use of sparse but specific image space information, such as calcified atherosclerotic plaque, can be used to substantially improve the performance of a previously described knowledge-based method to restore the centerlines of femoropopliteal arterial occlusions.
Figures






References
-
- Zarins C. K., Xu C., and Glagov S., “Artery wall pathology in atherosclerosis,” in: Vascular Surgery, 6th ed.(Saunders, Philadelphia, 2005), pp. 123–148.
-
- Roos J. E., Köechl A., Rakshe T., Straka M., Napoli A., Kanitsar A., Šrámek M., Gröller E., and Fleischmann D., “Multi-path curved planar reformation (mpCPR) of the peripheral arterial tree in CT angiography (CTA),” Radiology RADLAX 244, 281–290 (2007). - PubMed
-
- Kanitsar A., Wegenkittl R., Felkel P., Fleischmann D., Sandner D., and Gröeller E., “Computed tomography angiography: A case study of peripheral vessel investigation,” Proceedings of IEEE Visualization 2001, San Diego, California, pp. 477–480.
-
- Cohen L. D. and Deschamps T., “Grouping connected components using minimal path techniques: Application to reconstruction of vessels in 2D and 3D images,” IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR’01), 2001, pp. 102–109.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
