

Global eradication of lymphatic filariasis: the value of chronic disease control in parasite elimination programmes
- PMID: 18698350
- PMCID: PMC2490717
- DOI: 10.1371/journal.pone.0002936
Global eradication of lymphatic filariasis: the value of chronic disease control in parasite elimination programmes
Abstract
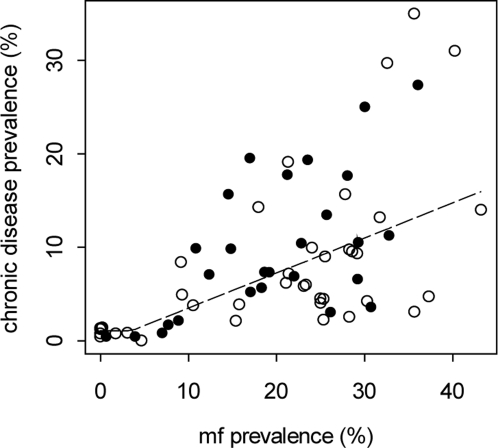
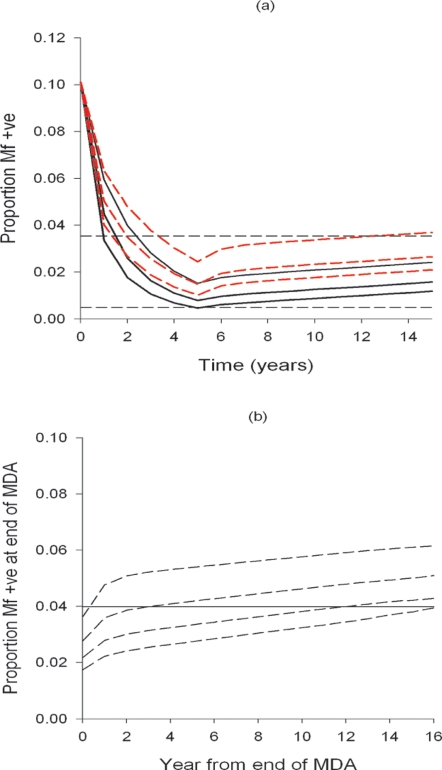
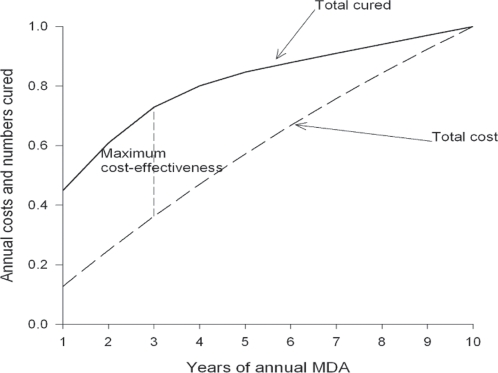
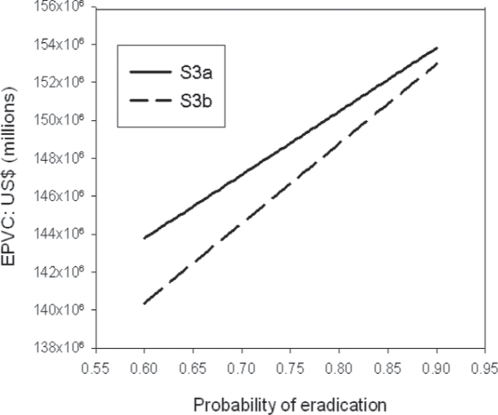
The ultimate goal of the global programme against lymphatic filariasis is eradication through irrevocable cessation of transmission using 4 to 6 years of annual single dose mass drug administration. The costs of eradication, managerial impediments to executing national control programmes, and scientific uncertainty about transmission endpoints, are challenges to the success of this effort, especially in areas of high endemicity where financial resources are limited. We used a combined analysis of empirical community data describing the association between infection and chronic disease prevalence, mathematical modelling, and economic analyses to identify and evaluate the feasibility of setting an infection target level at which the chronic pathology attributable to lymphatic filariasis--lymphoedema of the extremities and hydroceles--becomes negligible in the face of continuing transmission as a first stage option in achieving the elimination of this parasitic disease. The results show that microfilaria prevalences below a threshold of 3.55% at a blood sampling volume of 1 ml could constitute readily achievable and sustainable targets to control lymphatic filarial disease. They also show that as a result of the high marginal cost of curing the last few individuals to achieve elimination, maximal benefits can occur at this threshold. Indeed, a key finding from our coupled economic and epidemiological analysis is that when initial uncertainty regarding eradication occurs and prospects for resolving this uncertainty over time exist, it is economically beneficial to adopt a flexible, sequential, eradication strategy based on controlling chronic disease initially.
Conflict of interest statement
Figures
References
-
- Evans DB, Gelband H, Vlassoff C. Social and economic factors and the control of lymphatic filariasis: a review. Acta Trop. 1993;53:1–26. - PubMed
-
- Ramaiah KD, Das PK. Mass drug administration to eliminate lymphatic filariasis in India. Trends Parasitol. 2004;20:499–502. - PubMed
-
- Michael E, Malecela-Lazaro MN, Kabali C, Snow LC, Kazura JW. Mathematical models and lymphatic filariasis control: endpoints and optimal interventions. Trends Parasitol. 2006;22:226–233. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
