

Cognitive-behavioural therapy v. structured care for medically unexplained symptoms: randomised controlled trial
- PMID: 18700219
- PMCID: PMC2802526
- DOI: 10.1192/bjp.bp.107.043190
Cognitive-behavioural therapy v. structured care for medically unexplained symptoms: randomised controlled trial
Abstract
Background: A pilot trial in Sri Lanka among patients with medically unexplained symptoms revealed that cognitive-behavioural therapy (CBT) administered by a psychiatrist was efficacious.
Aims: To evaluate CBT provided by primary care physicians in a comparison with structured care.
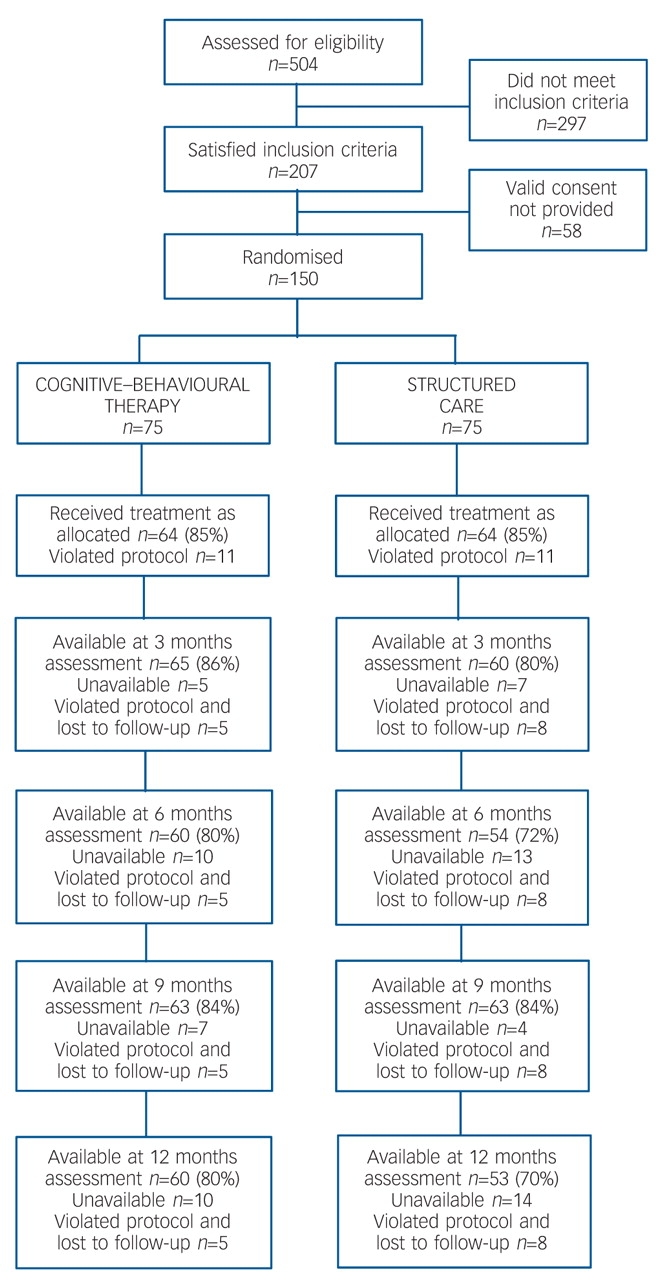
Method: A randomised control trial (n=75 in each arm) offered six 30 min sessions of structured care or therapy. The outcomes of the two interventions were compared at 3 months, 6 months, 9 months and 12 months.
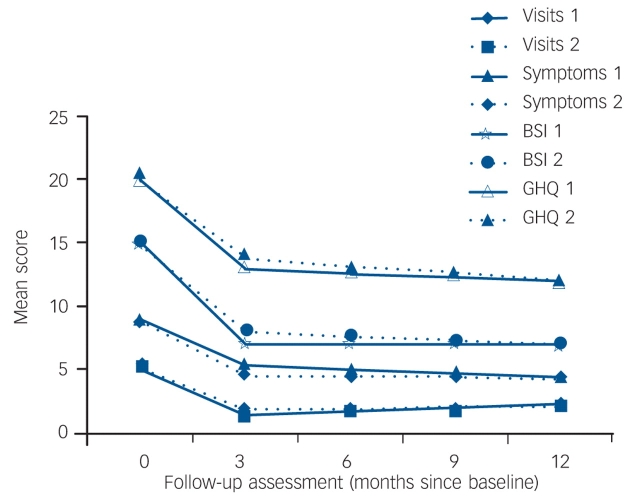
Results: In each arm, 64 patients (85%) completed the three mandatory sessions. No difference was observed between groups in mean scores on the General Health Questionnaire or the Bradford Somatic Inventory, or in number of complaints or patient-initiated consultations at 3 months. For both groups, all outcome measures improved at 3 months, and remained constant in the follow-up assessments.
Conclusions: Cognitive-behavioural therapy given by primary care physicians after a short course of training is no more efficacious than structured care. Natural remission is an unlikely explanation for improvements in people with chronic medically unexplained symptoms, but lack of a 'treatment as usual' arm limits further conclusions. Further research on enhanced structured care, medical assessment and structured care incorporating simple elements of CBT principles is worthy of consideration.
Figures
References
-
- Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med 1989; 86: 262–6. - PubMed
-
- Kroenke K, Price RK. Symptoms in the community: prevalence, classification, and psychiatric co-morbidity. Arch Intern Med 1993; 153: 2474–80. - PubMed
-
- Henningsen P, Zimmermann T, Sattel H. Medically unexplained physical symptoms, anxiety, and depression: a meta-analytic review. Psychosom Med 2003; 65: 528–33. - PubMed
-
- Toft T, Fink P, Oernboel E, Christensen K, Frostholm L, Olesen F. Mental disorders in primary care: prevalence and co-morbidity among disorders. Results from the Functional Illness in Primary care (FIP) study. Psychol Med 2005; 35: 1175–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
