

Treatment and outcome of Shiga-toxin-associated hemolytic uremic syndrome (HUS)
- PMID: 18704506
- PMCID: PMC6901419
- DOI: 10.1007/s00467-008-0935-6
Treatment and outcome of Shiga-toxin-associated hemolytic uremic syndrome (HUS)
Abstract
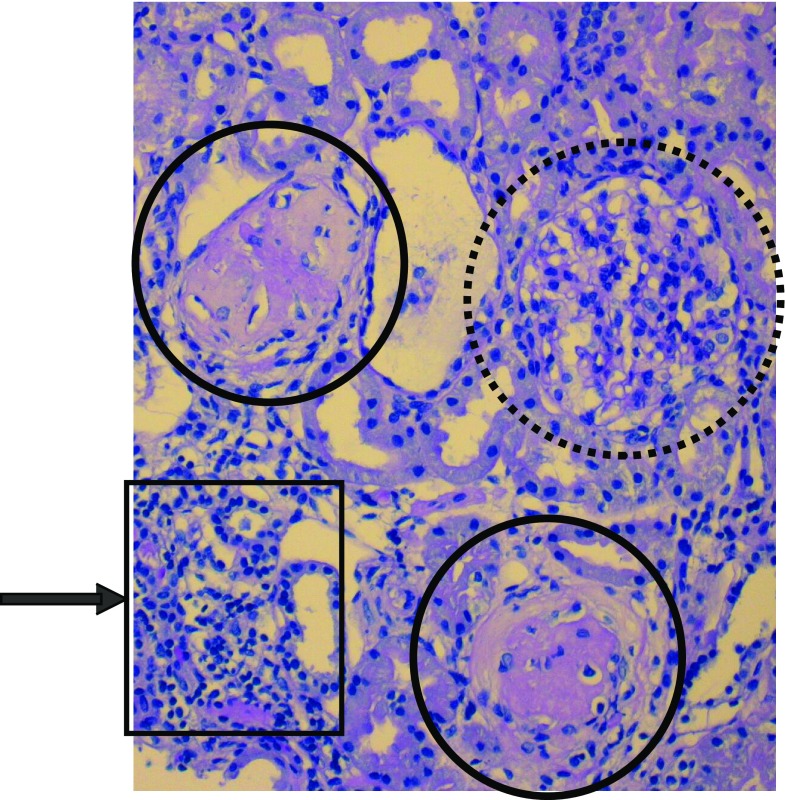
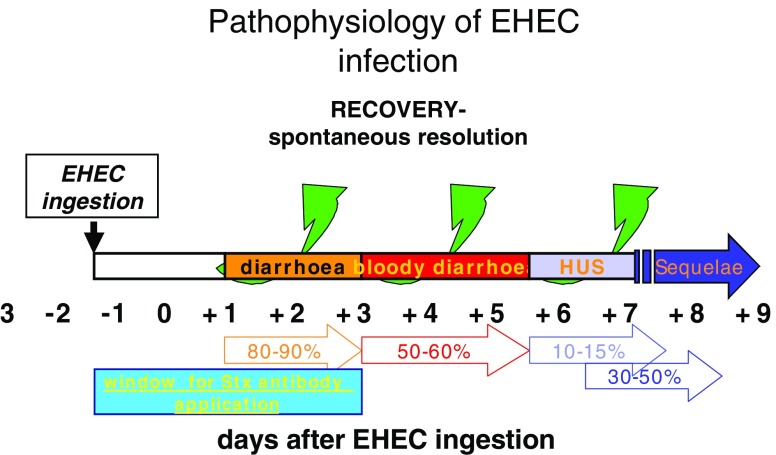
Hemolytic uremic syndrome (HUS) is the most common cause of acute renal failure in childhood and the reason for chronic renal replacement therapy. It leads to significant morbidity and mortality during the acute phase. In addition to acute morbidity and mortality, long-term renal and extrarenal complications can occur in a substantial number of children years after the acute episode of HUS. The most common infectious agents causing HUS are enterohemorrhagic Escherichia coli (EHEC)-producing Shiga toxin (and belonging to the serotype O157:H7) and several non-O157:H7 serotypes. D(+) HUS is an acute disease characterized by prodromal diarrhea followed by acute renal failure. The classic clinical features of HUS include the triad of microangiopathic hemolytic anemia, thrombocytopenia, and acute renal failure. HUS mortality is reported to be between 3% and 5%, and death due to HUS is nearly always associated with severe extrarenal disease, including severe central nervous system (CNS) involvement. Approximately two thirds of children with HUS require dialysis therapy, and about one third have milder renal involvement without the need for dialysis therapy. General management of acute renal failure includes appropriate fluid and electrolyte management, antihypertensive therapy if necessary, and initiation of renal replacement therapy when appropriate. The prognosis of HUS depends on several contributing factors. In general "classic" HUS, induced by EHEC, has an overall better outcome. Totally different is the prognosis in patients with atypical and particularly recurrent HUS. However, patients with severe disease should be screened for genetic disorders of the complement system or other underlying diseases.
Figures

References
-
- Zimmerhackl LB, Besbas N, Jungraithmayr T, van de Kar N, Karch H, Karpman D, Landau D, Loirat C, Proesmans W, Prufer F, Rizzoni G, Taylor MC. European study group for haemolytic uraemic syndromes and related disorders epidemiology, clinical presentation, and pathophysiology of atypical and recurrent haemolytic uraemic syndrome. Semin Thromb Hemost. 2006;32:113–120. doi: 10.1055/s-2006-939767. - DOI - PubMed
-
- Gerber A, Karch H, Allerberger F, Verweyen HM, Zimmerhackl LB. Clinical Course and the Role of Shiga Toxin Producing Escherichia coli infection in the haemolytic uraemic syndrome in pediatric patients, 1997–2000 in Germany and Austria: a prospective study. J Infect Dis. 2002;186:493–500. doi: 10.1086/341940. - DOI - PubMed
-
- Gasser C, Gautier E, Steck A, Siebenmann RE, Oechslin R. Hämolytisch-urämische Syndrom: Bilaterale Nierenrindennekrosen bei akuten erworbenen hämolytischen Anämien. Schweiz Med. Wochenschr. 1955;85:905–909. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
