

Combined sphingosine, S1P and ischemic postconditioning rescue the heart after protracted ischemia
- PMID: 18706887
- PMCID: PMC3402379
- DOI: 10.1016/j.bbrc.2008.08.022
Combined sphingosine, S1P and ischemic postconditioning rescue the heart after protracted ischemia
Abstract
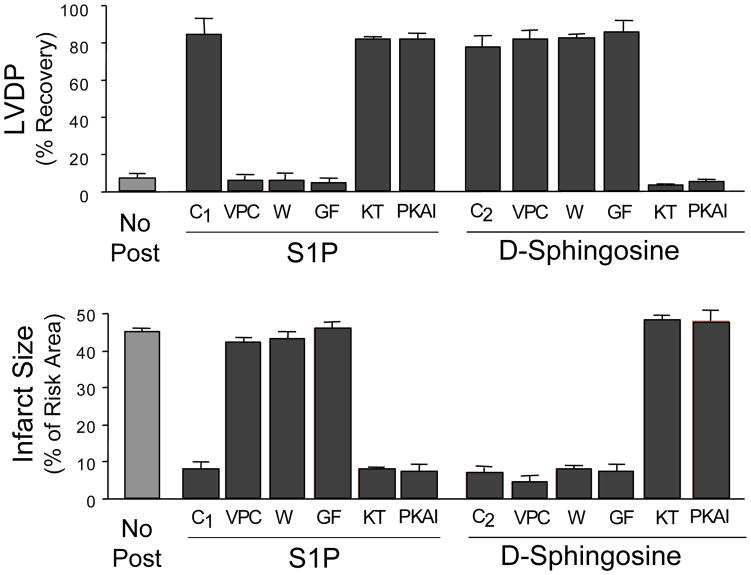
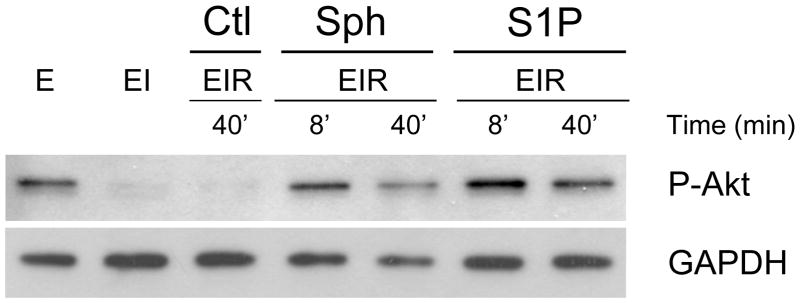
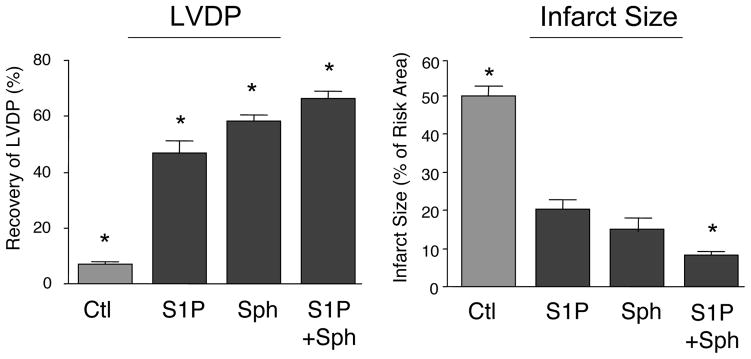
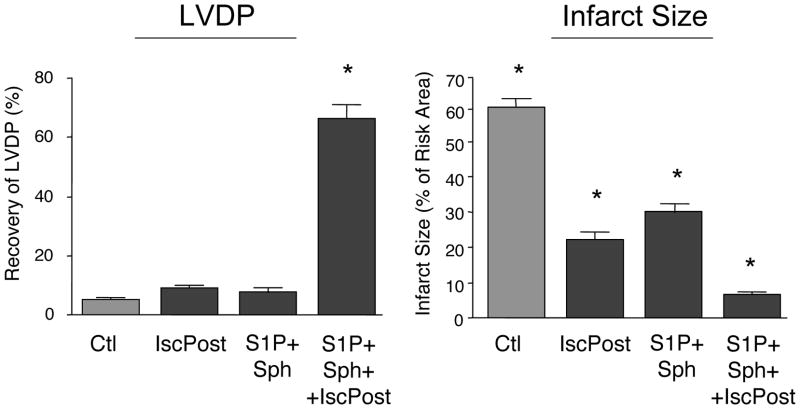
Both sphingosine and sphingosine-1-phosphate (S1P) were able to protect the ex vivo rat heart from ischemia reperfusion injury when added to the perfusion medium at the time of reperfusion after a 40min ischemia (postconditioning). Inhibitor studies revealed distinct mechanisms of protection, with S1P employing a G-protein coupled receptor pathway and sphingosine a cyclic nucleotide dependent protein kinase pathway. However, both restored ischemia-induced depletion of phospho-AKT. Extending the ischemia to 75min reduced protection by both S1P and sphingosine, but protection could be enhanced by employing them in combination. Extending the time of ischemia further to 90min almost eliminated cardioprotection by S1P or sphingosine; and their combination gave only modest protection. However, when S1P plus sphingosine was combined with a novel ramped ischemic postconditioning regimen, left ventricle developed pressure recovered by 66% and there was only a 6% infarct size. The data indicate that detrimental changes are accumulating during protracted ischemia but for up to 90min this damage is not irreversible and hearts can still recover with proper treatment.
Figures
References
-
- Jennings RB, Reimer KA. The Cell Biology of Acute Myocardial Ischemia. Ann Revs Med. 1991;42:225–246. - PubMed
-
- Buja LM, Entman ML. Modes of myocardial cell injury and cell death in ischemic heart disease. Circulation. 1998;98:1355–1357. - PubMed
-
- Hansen PR. Myocardial reperfusion injury: experimental evidence and clinical relevance. Eur Heart J. 1995;16:734–740. - PubMed
-
- Maxwell SR, Lip GY. Reperfusion injury: a review of the pathophysiology, clinical manifestations and therapeutic options. Int J Cardiol. 1997;58:95–117. - PubMed
-
- Zhao ZQ, Vinten-Johansen J. Myocardial apoptosis and ischemic preconditioning. Cardiovasc Res. 2002;55:438–455. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
