

Radiographic evaluation of bones and joints in mucopolysaccharidosis I and VII dogs after neonatal gene therapy
- PMID: 18707908
- PMCID: PMC2803678
- DOI: 10.1016/j.ymgme.2008.07.003
Radiographic evaluation of bones and joints in mucopolysaccharidosis I and VII dogs after neonatal gene therapy
Abstract
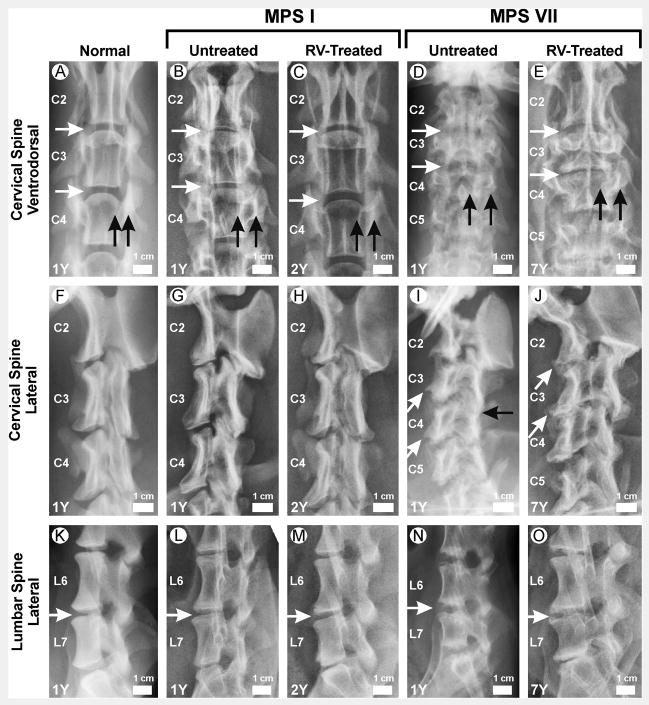
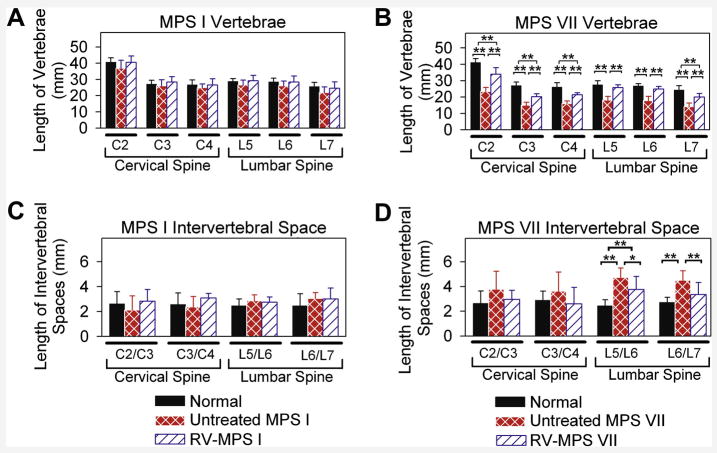
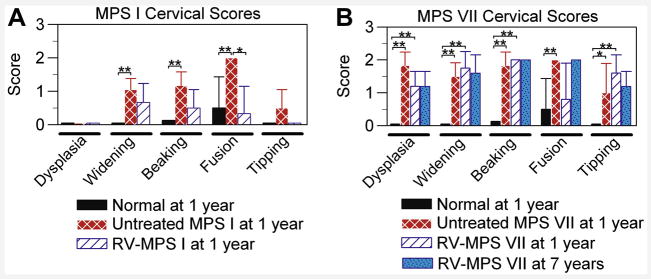
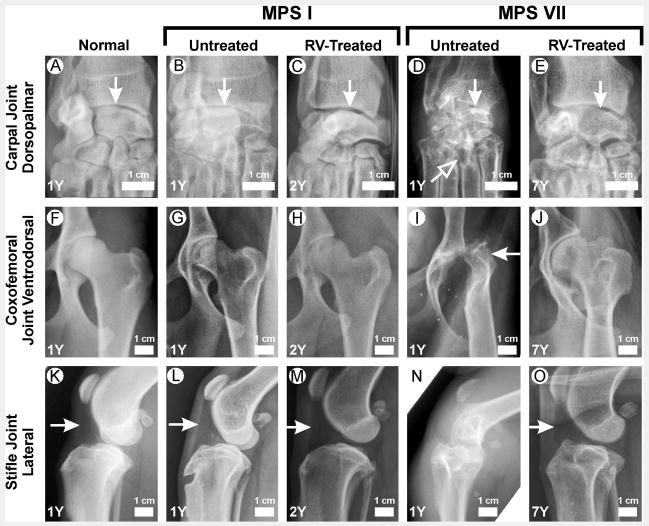
Mucopolysaccharidosis I (MPS I) and MPS VII are due to deficient activity of the glycosaminoglycan-degrading lysosomal enzymes alpha-L-iduronidase and beta-glucuronidase, respectively, and result in abnormal bones and joints. Here, the severity of skeletal disease in MPS I and MPS VII dogs and the effects of neonatal gene therapy were evaluated. For untreated MPS VII dogs, the lengths of the second cervical vertebrae (C2) and the femur were only 56% and 84% of normal, respectively, and bone dysplasia and articular erosions, and joint subluxation were severe. Previously, we reported that neonatal intravenous injection of a retroviral vector (RV) with the appropriate gene resulted in expression in liver and blood cells, and high serum enzyme activity. In this study, we demonstrate that C2 and femurs of RV-treated MPS VII dogs were longer at 82% and 101% of normal, respectively, and there were partial improvements of qualitative abnormalities. For untreated MPS I dogs, the lengths of C2 and femurs (91% and 96% of normal, respectively) were not significantly different from normal dogs. Qualitative changes in MPS I bones and joints were generally modest and were partially improved with RV treatment, although cervical spine disease was severe and was difficult to correct with gene therapy in both models. The greater severity of skeletal disease in MPS VII than in MPS I dogs may reflect accumulation of chondroitin sulfate in cartilage in MPS VII, or could relate to the specific mutations. Neonatal RV-mediated gene therapy ameliorates, but does not prevent, skeletal disease in MPS I and MPS VII dogs.
Figures


Similar articles
-
Neonatal retroviral vector-mediated hepatic gene therapy reduces bone, joint, and cartilage disease in mucopolysaccharidosis VII mice and dogs.Mol Genet Metab. 2004 May;82(1):4-19. doi: 10.1016/j.ymgme.2004.01.015. Mol Genet Metab. 2004. PMID: 15110316
-
The effect of neonatal gene therapy on skeletal manifestations in mucopolysaccharidosis VII dogs after a decade.Mol Genet Metab. 2013 Jun;109(2):183-93. doi: 10.1016/j.ymgme.2013.03.013. Epub 2013 Apr 6. Mol Genet Metab. 2013. PMID: 23628461 Free PMC article.
-
Gene therapy ameliorates cardiovascular disease in dogs with mucopolysaccharidosis VII.Circulation. 2004 Aug 17;110(7):815-20. doi: 10.1161/01.CIR.0000138747.82487.4B. Epub 2004 Aug 2. Circulation. 2004. PMID: 15289379
-
Murine mucopolysaccharidosis type VII: the impact of therapies on the clinical course and pathology in a murine model of lysosomal storage disease.J Inherit Metab Dis. 1998 Aug;21(5):575-86. doi: 10.1023/a:1005423222927. J Inherit Metab Dis. 1998. PMID: 9728337 Review.
-
Gene therapy for mucopolysaccharidosis.Expert Opin Biol Ther. 2007 Sep;7(9):1333-45. doi: 10.1517/14712598.7.9.1333. Expert Opin Biol Ther. 2007. PMID: 17727324 Free PMC article. Review.
Cited by
-
Effects of neonatal enzyme replacement therapy and simvastatin treatment on cervical spine disease in mucopolysaccharidosis I dogs.J Bone Miner Res. 2014 Dec;29(12):2610-7. doi: 10.1002/jbmr.2290. J Bone Miner Res. 2014. PMID: 24898323 Free PMC article.
-
Gene therapy for lysosomal storage diseases (LSDs) in large animal models.ILAR J. 2009;50(2):112-21. doi: 10.1093/ilar.50.2.112. ILAR J. 2009. PMID: 19293456 Free PMC article. Review.
-
Long-term amelioration of feline Mucopolysaccharidosis VI after AAV-mediated liver gene transfer.Mol Ther. 2011 Mar;19(3):461-9. doi: 10.1038/mt.2010.257. Epub 2010 Nov 30. Mol Ther. 2011. PMID: 21119624 Free PMC article.
-
Altered lumbar spine structure, biochemistry, and biomechanical properties in a canine model of mucopolysaccharidosis type VII.J Orthop Res. 2010 May;28(5):616-22. doi: 10.1002/jor.21030. J Orthop Res. 2010. PMID: 19918911 Free PMC article.
-
Large animal models of neurological disorders for gene therapy.ILAR J. 2009;50(2):128-43. doi: 10.1093/ilar.50.2.128. ILAR J. 2009. PMID: 19293458 Free PMC article. Review.
References
-
- Neufeld EF, Muenzer J. The Mucopolysaccharidoses. In: Scriver CR, Beaudet AL, Sly WS, Valle D, editors. Metabolic and Molecular Basis of Inherited Disease. New York: McGraw Hill; 2001. pp. 3421–3452.
-
- Poorthuis BJ, Wevers RA, Kleijer WJ, Groener JE, de Jong JG, van Weely S, Niezen-Koning KE, van Diggelen OP. The frequency of lysosomal storage diseases in The Netherlands. Hum Genet. 1999;105:151–156. - PubMed
-
- Masterson EL, Murphy PG, O’Meara A, Moore DP, Dowling FE, Fogarty EE. Hip dysplasia in Hurler’s syndrome: orthopedic management after bone marrow transplantation. J Ped Ortho. 1996;16:731–733. - PubMed
-
- Stevenson RE, Howell RR, McKusick VA, Suskind R, Hanson JW, Elliott DE, Neufeld EF. The iduronidase-deficient mucopolysaccharidoses: clinical and roentgenographic features. Pediatrics. 1976;57:111–122. - PubMed
-
- Tandon V, Williamson JB, Cowie RA, Wraith JE. Spinal problems in mucopolysaccharidosis I (Hurler syndrome) J Bone Joint Surg Br. 1996;78:938–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
