

Unravelling the pathophysiology of delirium: a focus on the role of aberrant stress responses
- PMID: 18707945
- PMCID: PMC4311661
- DOI: 10.1016/j.jpsychores.2008.05.019
Unravelling the pathophysiology of delirium: a focus on the role of aberrant stress responses
Abstract
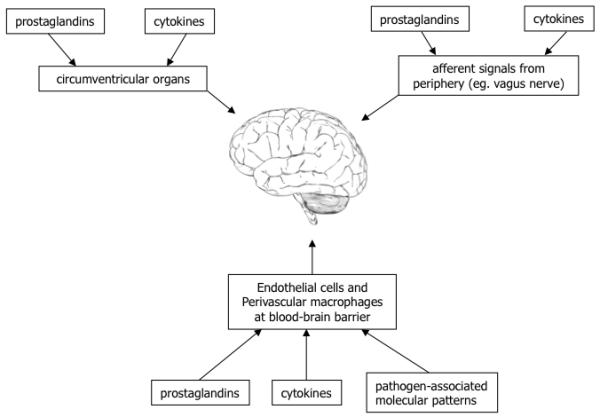
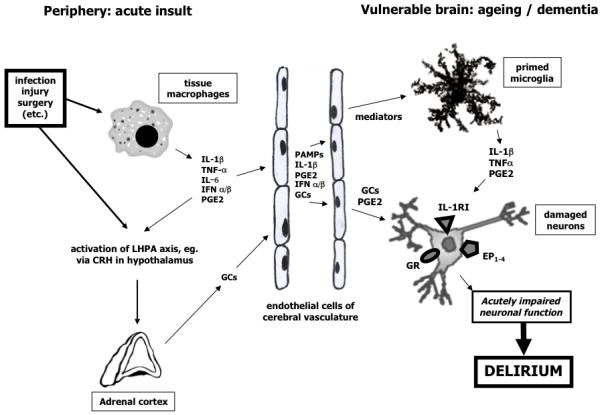
Delirium is a common and serious acute neuropsychiatric syndrome with core features of inattention and cognitive impairment, and associated features including changes in arousal, altered sleep-wake cycle, and other changes in mental status. The main risk factors are old age, cognitive impairment, and other comorbidities. Though delirium has consistent core clinical features, it has a very wide range of precipitating factors, including acute illness, surgery, trauma, and drugs. The molecular mechanisms by which these precipitating factors lead to delirium are largely obscure. In this article, we attempt to narrow down some specific causal pathways. We propose a basic classification for the etiological factors: (a) direct brain insults and (b) aberrant stress responses. Direct brain insults are largely indiscriminate and include general and regional energy deprivation (e.g., hypoxia, hypoglycaemia, stroke), metabolic abnormalities (e.g., hyponatraemia, hypercalcaemia), and the effects of drugs. Aberrant stress responses are conceptually and mechanistically distinct in that they constitute adverse effects of stress-response pathways, which, in health, are adaptive. Ageing and central nervous system disease, two major predisposing factors for delirium, are associated with alterations in the magnitude or duration of stress and sickness behavior responses and increased vulnerability to the effects of these responses. We discuss in detail two stress response systems that are likely to be involved in the pathophysiology of delirium: inflammation and the sickness behavior response, and activity of the limbic-hypothalamic-pituitary-adrenal axis. We conclude by discussing the implications for future research and the development of new therapies for delirium.
Figures
References
-
- Meagher DJ, Moran M, Raju B, Gibbons D, Donnelly S, Saunders J, Trzepacz PT. Phenomenology of delirium - Assessment of 100 adult cases using standardised measures. British Journal of Psychiatry. 2007;190:135–41. - PubMed
-
- Trzepacz PT, Baker RW, Greenhouse J. A symptom rating-scale for delirium. Psychiatry Research. 1988;23(1):89–97. - PubMed
-
- Inouye SK, Charpentier PA. Precipitating factors for delirium in hospitalized elderly persons - Predictive model and interrelationship with baseline vulnerability. JAMA - Journal of the American Medical Association. 1996;275(11):852–7. - PubMed
-
- Marcantonio ER, Goldman L, Mangione CM, Ludwig LE, Muraca B, Haslauer CM, Donaldson MC, Whittemore AD, Sugarbaker DJ, Poss R, Haas S, Cook EF, Orav J, Lee TH. A clinical-prediction rule for delirium after elective noncardiac surgery. JAMA-Journal of the American Medical Association. 1994;271(2):134–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
