

Hepatic neuroendocrine metastases: chemo- or bland embolization?
- PMID: 18709512
- PMCID: PMC3342849
- DOI: 10.1007/s11605-008-0640-6
Hepatic neuroendocrine metastases: chemo- or bland embolization?
Abstract
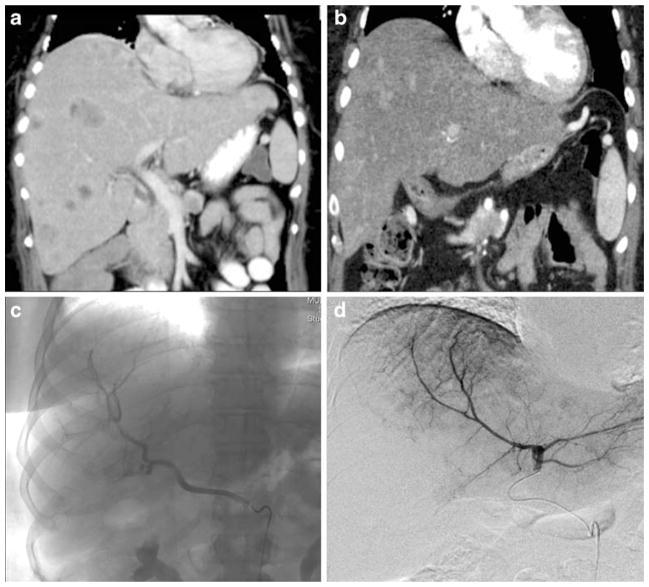
Introduction: Aggressive management of hepatic neuroendocrine (NE) metastases improves symptoms and prolongs survival. Because of the rarity of these tumors, however, the best method for hepatic artery embolization has not been established. We hypothesized that in patients with hepatic NE metastases, hepatic artery chemoembolization (HACE) would result in better symptom improvement and survival compared to bland embolization (HAE).
Methods: Retrospective review identified all patients with NE hepatic metastases managed by HACE or HAE at three institutions from January 1996 through December 2007.
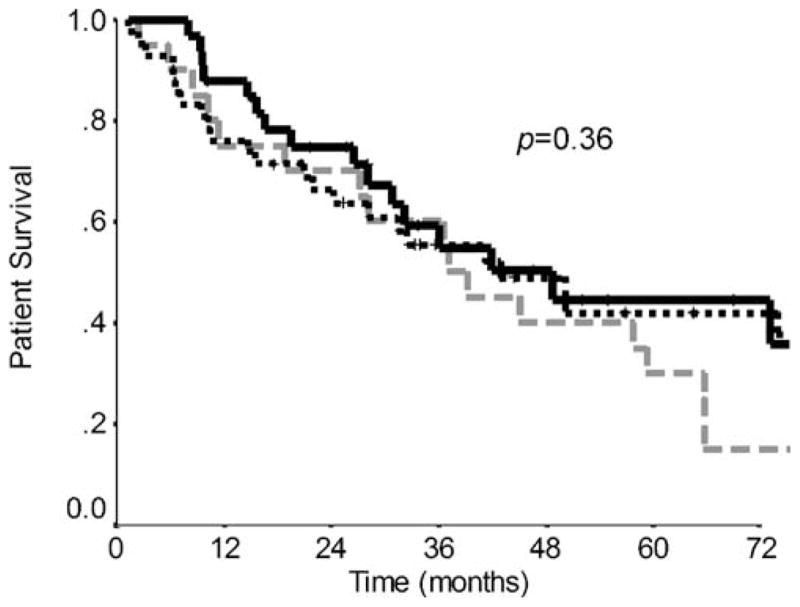
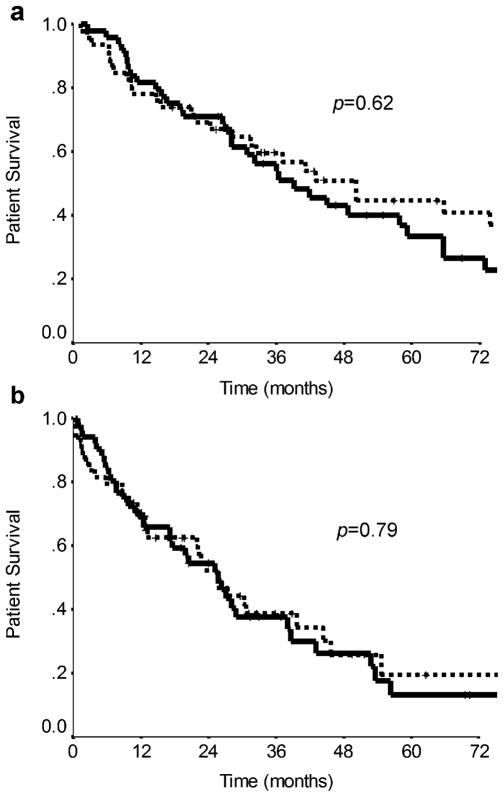
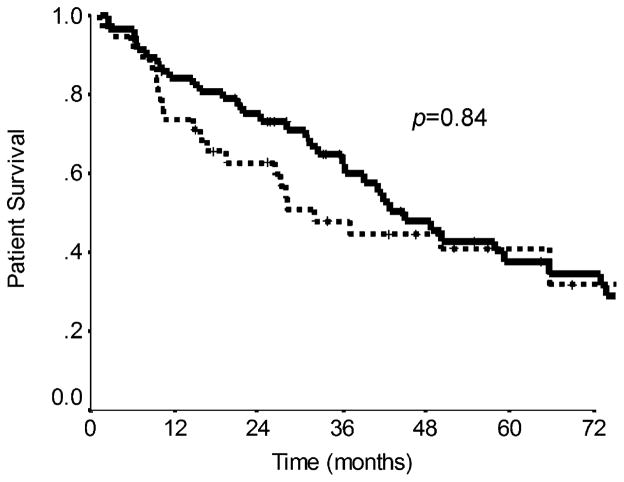
Results: We identified 100 patients managed by HACE (n = 49) or HAE (n = 51) that were similar with respect to age, gender, and primary tumor type. The percentage of patients experiencing morbidity, 30-day mortality, and symptom improvement were similar between the two groups (HACE vs. HAE: 2.4% vs. 6.6%; 0.8% vs. 1.8%; and 88% vs. 83%, respectively.) No differences in the median overall survival were observed between HACE and HAE from the time of the first embolization procedure (25.5 vs. 25.7 months, p = 0.79). Multivariate analysis revealed that resection of the primary tumor predicted survival (73.8 vs. 19.4 months, p < 0.04).
Conclusions: These data suggest that morbidity, mortality, symptom improvement, and overall survival are similar in patients with hepatic neuroendocrine metastases managed by chemo- or bland hepatic artery embolization.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
