

Association of chronic kidney disease with outcomes in chronic heart failure: a propensity-matched study
- PMID: 18711222
- PMCID: PMC2721423
- DOI: 10.1093/ndt/gfn445
Association of chronic kidney disease with outcomes in chronic heart failure: a propensity-matched study
Abstract
Background: Chronic kidney disease (CKD) is associated with increased mortality in patients with heart failure (HF). However, its association with hospitalization in HF patients has not been well studied.
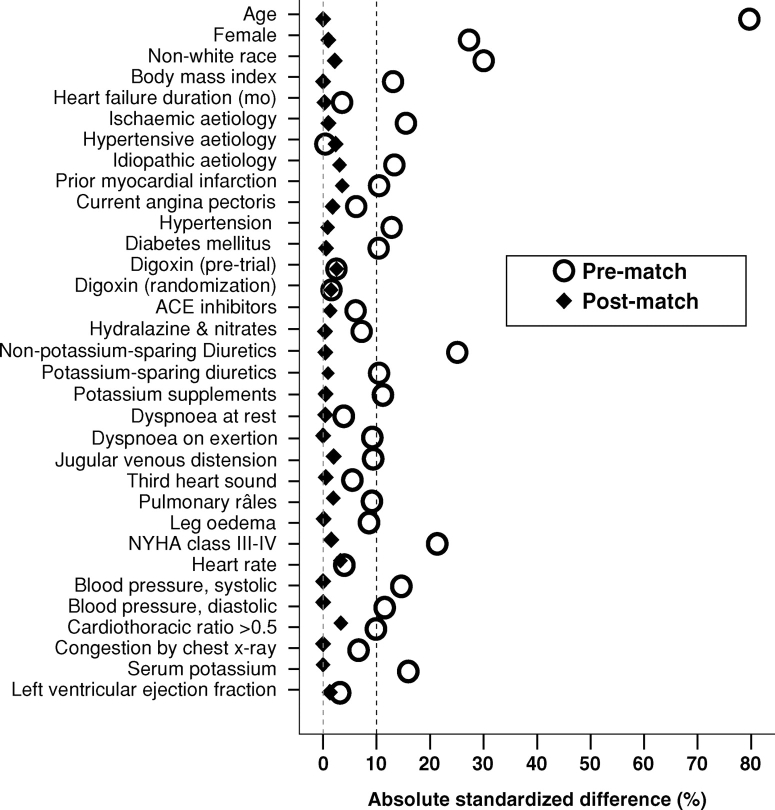
Methods: Of 7788 patients in the Digitalis Investigation Group trial, 3527 had CKD, defined by an estimated glomerular filtration rate (GFR) <60 ml/min/1.73 m(2) body surface area (BSA). Propensity scores for CKD were calculated using a multivariable logistic regression model and used to match 2399 pairs of patients with and without CKD. Matched Cox regression analyses were used to estimate association of CKD with outcomes.
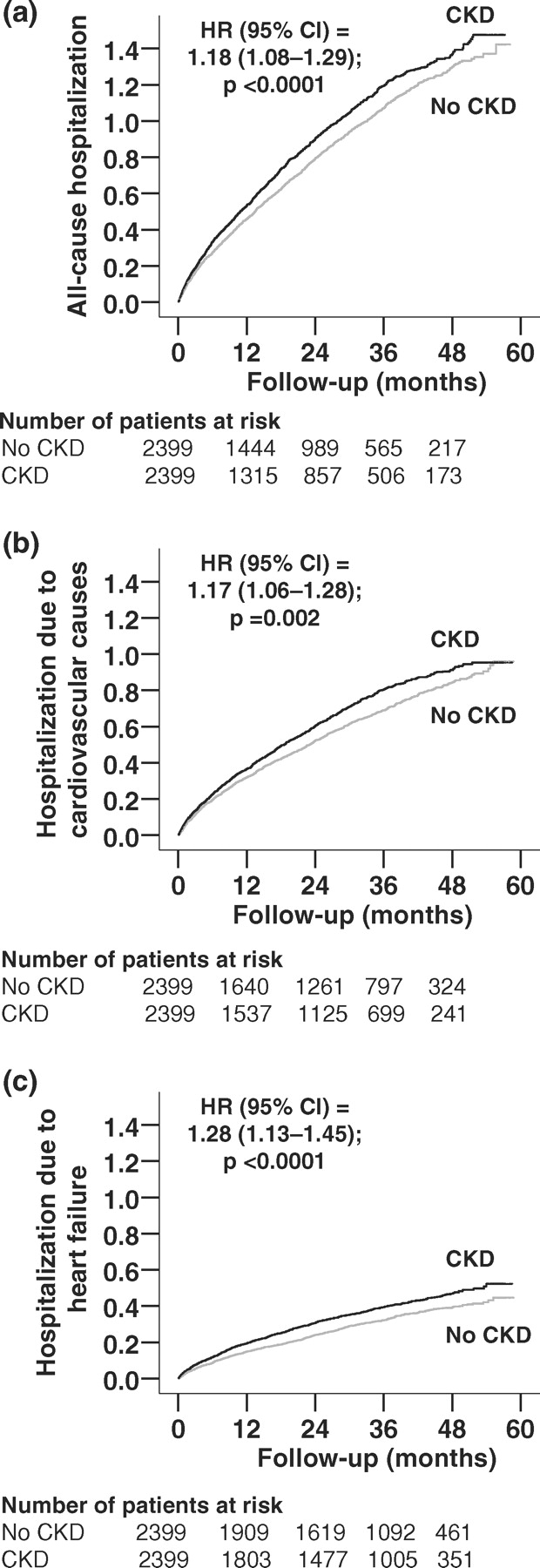
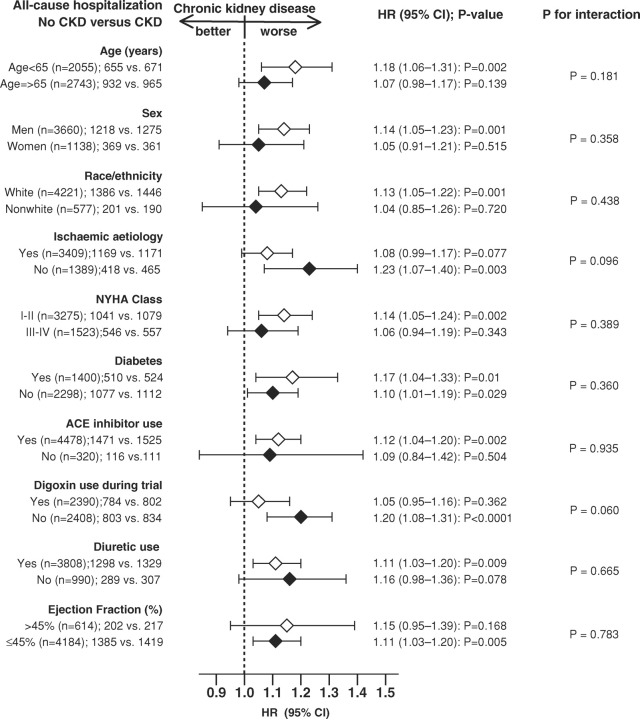
Results: All-cause hospitalization occurred in 1636 (rate, 4233/10,000 person-years) and 1587 (rate, 3733/10,000 person-years) patients respectively, with and without CKD (matched hazard ratio [HR] for CKD, 1.18, 95% confidence interval [CI], 1.08-1.29; P < 0.0001). Matched HR for cardiovascular and HF hospitalization were respectively 1.17 (95% CI, 1.06-1.28, P = 0.002) and 1.28 (95% CI, 1.13-1.45, P < 0.0001). Compared to GFR >or=60 ml/min/1.73 m(2) BSA, HR for all-cause hospitalization for GFR 45-59 and <45 ml/min/1.73 m(2) BSA were respectively 1.04 (95% CI, 0.94-1.16; P = 0.422) and 1.58 (95% CI, 1.34-1.87; P < 0.0001). Similarly, HR for all-cause death for GFR 45-59 and <45 ml/min/1.73 m(2) BSA were respectively 1.03 (95% CI, 0.90-1.18; P = 0.651) and 1.70 (95% CI, 1.40-2.07; P < 0.0001). Matched HR for death due to cardiovascular causes and progressive HF were respectively 1.24 (95% CI, 1.09-1.40; P = 0.001) and 1.42 (95% CI, 1.16-1.72; P = 0.001).
Conclusion: CKD was associated with increased mortality and hospitalization in ambulatory patients with chronic HF, which increased progressively with worsening kidney function.
Figures
References
-
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics—2007 update: a report from the American heart association statistics committee and stroke statistics subcommittee. Circulation. 2007;115:e69–e171. - PubMed
-
- Coresh J, Astor BC, Greene T, et al. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: third national health and nutrition examination survey. Am J Kidney Dis. 2003;41:1–12. - PubMed
-
- Ahmed A, Kiefe CI, Allman RM, et al. Survival benefits of angiotensin-converting enzyme inhibitors in older heart failure patients with perceived contraindications. J Am Geriatr Soc. 2002;50:1659–1666. - PubMed
-
- Mahon NG, Blackstone EH, Francis GS, et al. The prognostic value of estimated creatinine clearance alongside functional capacity in ambulatory patients with chronic congestive heart failure. J Am Coll Cardiol. 2002;40:1106–1113. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
