

Response criteria for glioma
- PMID: 18711427
- PMCID: PMC4795821
- DOI: 10.1038/ncponc1204
Response criteria for glioma
Abstract
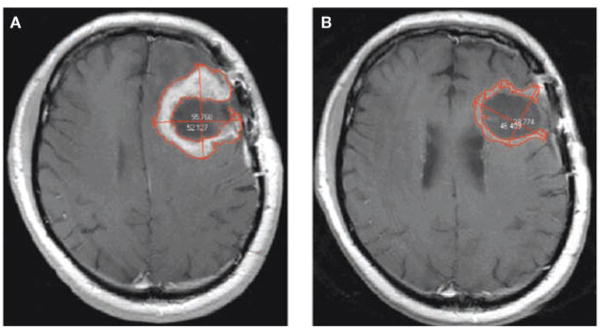
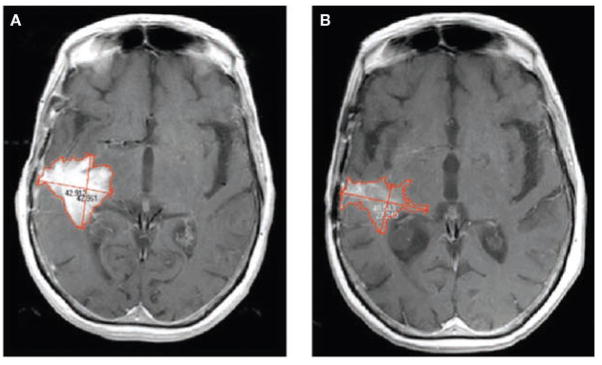
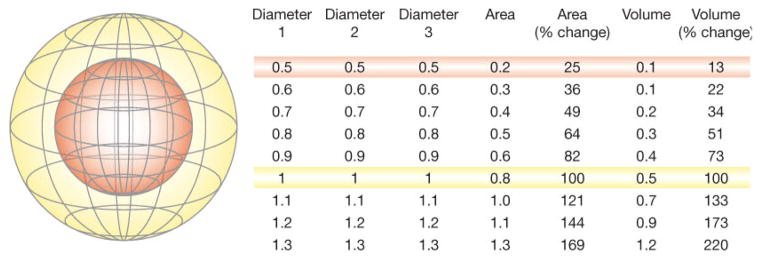
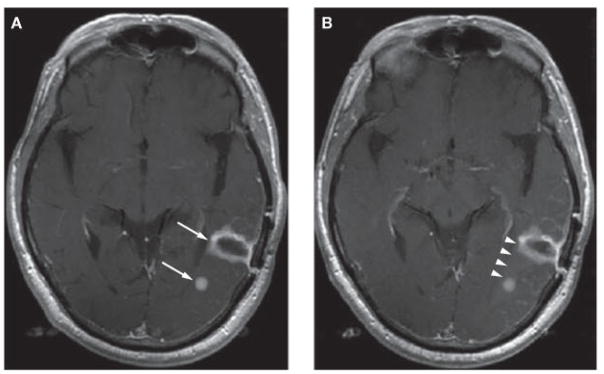
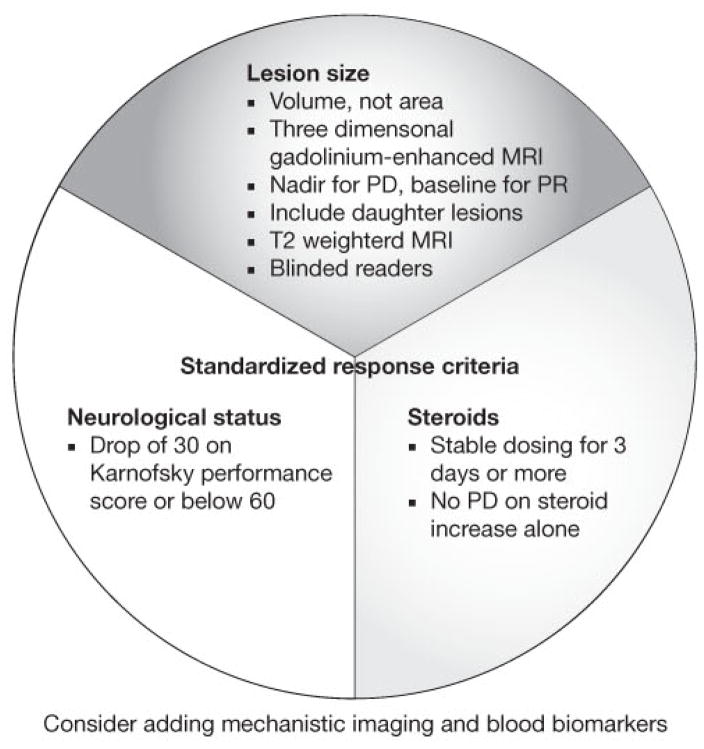
The current method for assessing the response to therapy of glial tumors was described by Macdonald et al. in 1990. Under this paradigm, response categorization is determined on the basis of changes in the cross-sectional area of a tumor on neuroimaging, coupled with clinical assessment of neurological status and corticosteroid utilization. These categories of response have certain limitations; for example, cross-sectional assessment is not as accurate as volumetric assessment, which is now feasible. Disentangling antitumor effects of therapies from their effects on blood-brain barrier permeability can be challenging. The use of insufficient response criteria might be overestimating the true benefits of drugs in early-stage studies, and, therefore, such therapies could mistakenly move forward into later phases, only to result in disappointment when overall survival is measured. We propose that studies report both radiographic and clinical response rates, use volumetric rather than cross-sectional area to measure lesion size, and incorporate findings from mechanistic imaging and blood biomarker studies more frequently, and also suggest that investigators recognize the limitations of imaging biomarkers as surrogate end points.
Conflict of interest statement
AG Sorensen declared associations with the following companies and organizations: ACR ImageMetrix, Amgen, AstraZeneca, Breakaway Imaging, Bayer–Schering, Eli Lilly, EPIX Pharmaceuticals, Exelixis, Genentech, General Electric Healthcare, Mitsubishi Pharma, National Institutes of Health, Novartis, Northwest Biosciences, Pfizer, Schering–Plough, Siemens Medical Solutions, Takeda-Millennium and Thermal Technologies Inc. TT Batchelor declared associations with the following companies: Enzon and Schering–Plough. RK Jain declared associations with the following companies: AstraZeneca, Dyax and SynDevRx. PY Wen declared associations with the following companies: Amgen, AstraZeneca, Exelixis, Genentech, Novartis and Schering–Plough. See the article online for full details of the relationships. W-T Zhang declared no competing interests.
Figures
References
-
- The Online NewsHour (online 28 March 2007) Extended interview: Janet Woodcock discusses cancer biomarkers. [accessed 28 April 2007]; http://www.pbs.org/newshour/bb/health/jan-june07/cancerwoodcock_03-28.html.
-
- Woodcock J. [accessed 28 April 2007];The Critical Path initiative: one year later. online 5 May 2005. www.fda.gov/cder/regulatory/medlmaging/woodcock.ppt.
-
- Johnson JR, et al. End points and United States Food and Drug Administration approval of oncology drugs. J Clin Oncol. 2003;21:1404–1411. - PubMed
-
- Macdonald DR, et al. Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol. 1990;8:1277–1280. - PubMed
-
- Brada M, Yung WK. Clinical trial end points in malignant glioma: need for effective trial design strategy. Semin Oncol. 2000;27:11–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical