

Evidence for increased postprandial distal nephron calcium delivery in hypercalciuric stone-forming patients
- PMID: 18715937
- PMCID: PMC2584913
- DOI: 10.1152/ajprenal.90404.2008
Evidence for increased postprandial distal nephron calcium delivery in hypercalciuric stone-forming patients
Abstract
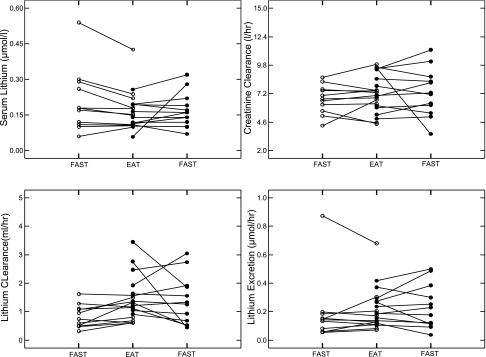
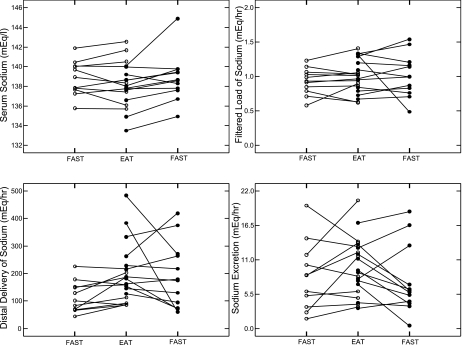
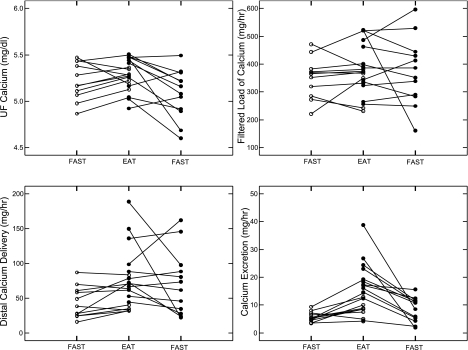
A main mechanism of idiopathic hypercalciuria (IH) in calcium stone-forming patients (IHSF) is postprandial reduction of renal tubule calcium reabsorption that cannot be explained by selective reduction of serum parathyroid hormone levels; the nephron site(s) responsible are not as yet defined. Using fourteen 1-h measurements of the clearances of sodium, calcium, and endogenous lithium during a three-meal day in the University of Chicago General Clinical Research Center, we found reduced postprandial proximal tubule reabsorption of sodium and calcium in IHSF vs. normal subjects. The increased distal sodium delivery is matched by increased distal reabsorption so that urine sodium excretions do not differ, but distal calcium reabsorption does not increase enough to match increased calcium delivery, so hypercalciuria results. In fact, urine calcium excretion and overall renal fractional calcium reabsorption both are high in IHSF vs. normal when adjusted for distal calcium delivery, strongly suggesting a distal as well as proximal reduction of calcium reabsorption. The combination of reduced proximal tubule and distal nephron calcium reabsorption in IHSF is a new finding and indicates that IH involves a complex, presumably genetic, variation of nephron function. The increased calcium delivery into the later nephron may play a role in stone formation via deposition of papillary interstitial apatite plaque.
Figures

References
-
- Ba J, Friedman PA. Calcium-sensing receptor regulation of renal mineral ion transport. Cell Calcium 35: 229–237, 2004. - PubMed
-
- Burnier M, Biollaz J, Magnin JL, Bidlingmeyer M, Brunner HR. Renal sodium handling in patients with untreated hypertension and white coat hypertension. Hypertension 23: 496–502, 1994. - PubMed
-
- Chiolero A, Maillard M, Nussberger J, Brunner HR, Burnier M. Proximal sodium reabsorption: an independent determinant of blood pressure response to salt. Hypertension 36: 631–637, 2000. - PubMed
-
- Diggle P, Heagerty P, Liang K, Zeger S. Analysis of Longitudinal Data. Oxford: Oxford University Press, 2002.
-
- Evan AP, Coe FL, Lingeman JE, Shao Y, Sommer AJ, Bledsoe SB, Anderson JC, Worcester EM. Mechanism of formation of human calcium oxalate renal stones on Randall's plaque. Anat Rec (Hoboken) 290: 1315–1323, 2007. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical