

Aldose reductase genotypes and cardiorenal complications: an 8-year prospective analysis of 1,074 type 2 diabetic patients
- PMID: 18716049
- PMCID: PMC2571065
- DOI: 10.2337/dc08-0712
Aldose reductase genotypes and cardiorenal complications: an 8-year prospective analysis of 1,074 type 2 diabetic patients
Abstract
Objective: We report the independent risk association of type 2 diabetic nephropathy with the z-2 allele of the 5'-(CA)(n) microsatellite and C-106T promoter polymorphisms of the aldose reductase gene (ALR2) using a case-control design. In this expanded cohort, we examined their predictive roles on new onset of cardiorenal complications using a prospective design.
Research design and methods: In this 8-year prospective cohort of 1,074 type 2 diabetic patients (59% male, median age 61 years; disease duration 7 years) with an observation period of 8,592 person-years, none had clinical evidence of coronary heart disease (CHD) or chronic kidney disease at recruitment. The renal end point was defined as new onset of estimated glomerular filtration rate <60 ml/min per 1.72 m(2) or hospitalizations with dialysis or death due to renal disease, and CHD was defined as hospitalizations with myocardial infarction, ischemic heart disease, or related deaths.
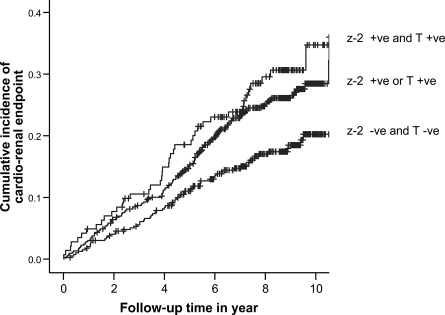
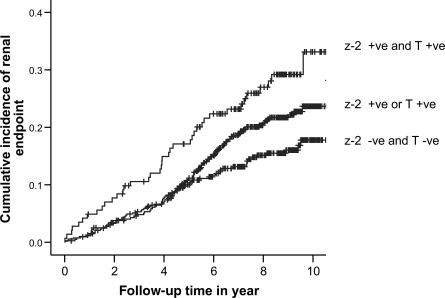
Results: After controlling for baseline risk factors and use of medications, we found that the ALR2 z-2 allele of (CA)(n) microsatellite carriers had increased risk of renal (hazard ratio 1.53 [95% CI 1.14-2.05], P = 0.005) or combined cardiorenal (1.31 [1.01-1.72], P = 0.047) end points. Carriers of the ALR2 C-106T polymorphism also had increased risk of renal (1.54 [1.15-2.07], P = 0.004) and cardiorenal (1.49 [1.14-1.95], P = 0.004) end points. Compared with noncarriers, patients with two risk-conferring genotypes had a twofold increased risk of renal (2.41 [1.57-3.70], P < 0.001) and cardiorenal (1.94 [1.29-2.91], P = 0.002) end points.
Conclusions: In Chinese type 2 diabetic patients, genetic polymorphisms of ALR2 independently predicted new onset of renal and cardiorenal end points, with the latter being largely mediated through renal disease.
Figures
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ, Parfrey P, Pfeffer M, Raij L, Spinosa DJ, Wilson PW: Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 108:2154–2169, 2003 - PubMed
-
- Adler AI, Stevens RJ, Manley SE, Bilous RW, Cull CA, Holman RR: Development and progression of nephropathy in type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int 63:225–232, 2003 - PubMed
-
- Fioretto P, Steffes MW, Sutherland DE, Goetz FC, Mauer M: Reversal of lesions of diabetic nephropathy after pancreas transplantation. N Engl J Med 339:69–75, 1998 - PubMed
-
- Schrijvers BF, De Vriese AS, Flyvbjerg A: From hyperglycemia to diabetic kidney disease: the role of metabolic, hemodynamic, intracellular factors and growth factors/cytokines. Endocr Rev 25:971–1010, 2004 - PubMed
-
- Wang Y, Ng MCY, Lee SC, So WY, Tong CY, Cockram CS, Critchley JAJH, Chan JCN: Phenotypic heterogeneity associations of two aldose reductase gene polymorphisms with nephropathy and retinopathy in type 2 diabetes. Diabetes Care 26:2410–2415, 2003 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
