

Methods of advanced wound management for care of combined traumatic and chemical warfare injuries
- PMID: 18716652
- PMCID: PMC2481389
Methods of advanced wound management for care of combined traumatic and chemical warfare injuries
Abstract
Objective: Chemical warfare agents are potential threats to military personnel and civilians. The potential for associated traumatic injuries is significant. Damage control surgery could expose medical personnel to agents contaminating the wounds. The objectives of this study were to demonstrate efficacy of surgical decontamination and assess exposure risk to attending personnel.
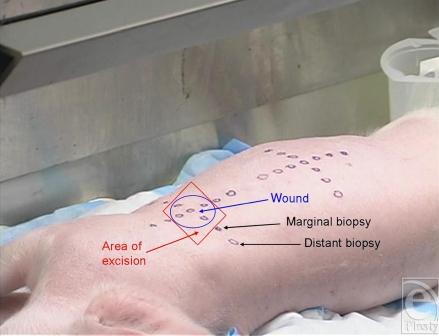
Methods: Weanling pigs were randomly assigned to 2 of 4 debridement tools (scalpel, Bovie knife, Fugo Blade, and Versajet Hydrosurgery System). Penetrating traumatic wounds were created over the shoulder and thigh and then exposed to liquid sulfur mustard (HD) for 60 minutes. Excisional debridement of the injuries was performed while vapors over each site were collected. Gas chromatography was used to measure HD in samples of collected vapors. Unbound HD was quantified in presurgical wound swabs, excised tissues, and peripheral tissue biopsies following solvent extraction.
Results: Excisional debridement produced agent-free wound beds (surgical decontamination). A significant amount of HD vapor was detected above the surgical fields with each tool. Apart from the Versajet producing significantly lower levels of HD detected over thigh wounds compared with those treated using the scalpel, there were no differences in the amount of agent detected among the tools. All measured levels significantly exceeded established safety limits. Vesicating levels of unbound HD were extracted from excised tissue. There was no measured lateral spreading of HD beyond the surgical margins.
Conclusions: There is significant occupational exposure risk to HD during surgical procedures designed to stabilize agent-contaminated wounds. If appropriate protective measures are taken, surgical decontamination is both effective and safe.
Figures





References
-
- Eastridge BJ, Jenkins D, Flaherty S, Schiller H, Holcomb JB. Trauma system development in a theater of war: experiences from Operation Iraqi Freedom and Operation Enduring Freedom. J Trauma. 2006;61(6):1366–73. - PubMed
-
- Chambers LW, Green DJ, Gillingham BL, et al. The experience of the US Marine Corp's surgical shock trauma platoon with 417 operative combat casualties during a 12 month period of Operation Iraqi Freedom. J Trauma. 2006;60(6):1155–64. - PubMed
-
- Perkins JG, Schreiber MA, Wade CE, Holcomb JB. Early versus late recombinant Factor VIIa in combat trauma patients requiring massive transfusion. J Trauma. 2007;62(5):1095–99. Discussion, 1099–1101. - PubMed
-
- Acosta JA, Hatzigeorgiou C, Smith LS. Developing a trauma registry in a forward deployed military hospital: preliminary report. J Trauma. 2006;61(2):256–60. - PubMed
-
- Leininger BE, Rasmussen TE, Smith DL, Jenkins DH, Coppola C. Experience with wound VAC and delayed primary closure of contaminated soft tissue injuries in Iraq. J Trauma. 2006;61(5):1207–11. - PubMed
LinkOut - more resources
Full Text Sources