

Ambulatory continuous posterior lumbar plexus nerve blocks after hip arthroplasty: a dual-center, randomized, triple-masked, placebo-controlled trial
- PMID: 18719448
- PMCID: PMC2590635
- DOI: 10.1097/ALN.0b013e318182a4a3
Ambulatory continuous posterior lumbar plexus nerve blocks after hip arthroplasty: a dual-center, randomized, triple-masked, placebo-controlled trial
Abstract
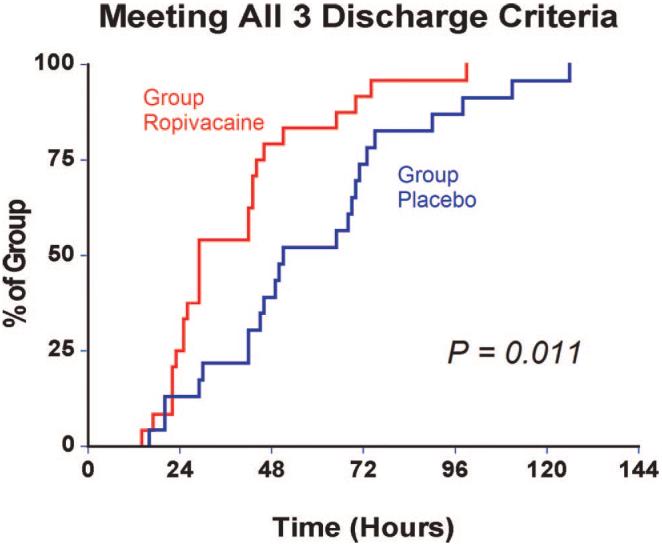
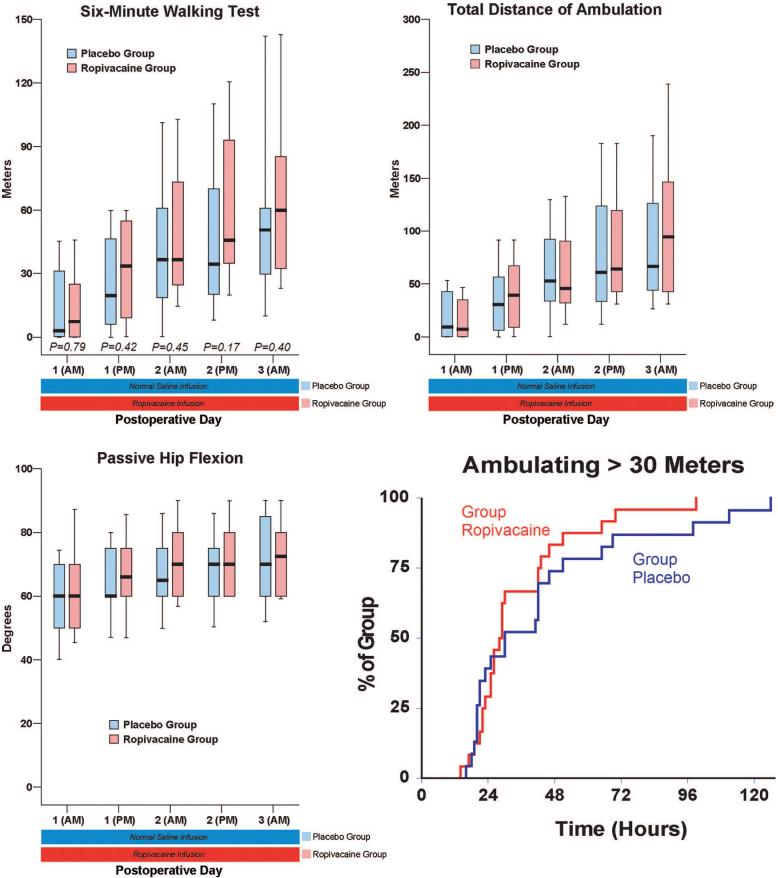
Background: The authors tested the hypotheses that after hip arthroplasty, ambulation distance is increased and the time required to reach three specific readiness-for-discharge criteria is shorter with a 4-day ambulatory continuous lumbar plexus block (cLPB) than with an overnight cLPB.
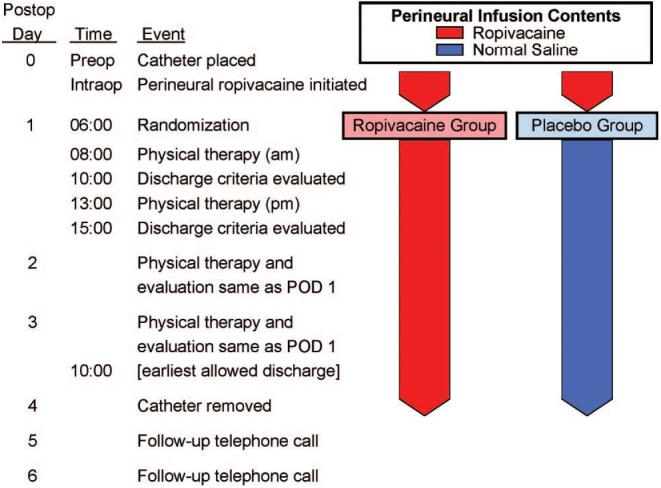
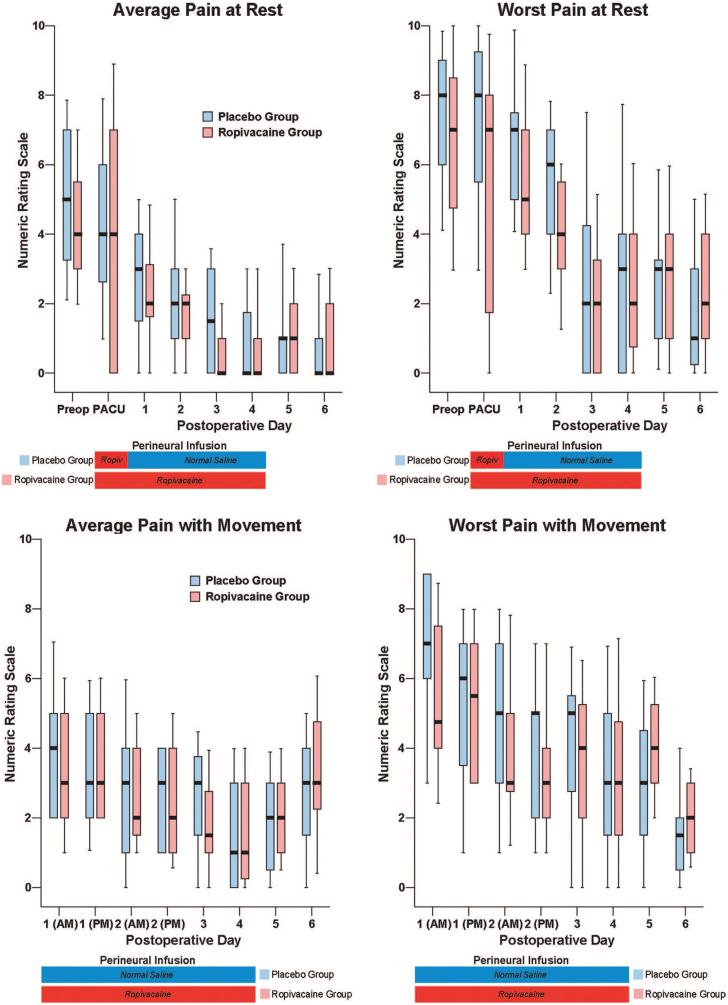
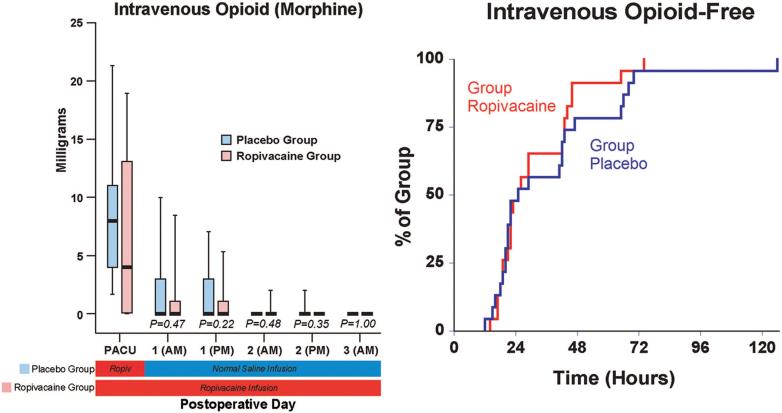
Methods: A cLPB consisting of 0.2% ropivacaine was provided from surgery until the following morning. Patients were then randomly assigned either to continue ropivacaine or to be switched to normal saline. Primary endpoints included (1) time to attain three discharge criteria (adequate analgesia, independence from intravenous analgesics, and ambulation > or = 30 m) and (2) ambulatory distance in 6 min the afternoon after surgery. Patients were discharged with their cLPB and a portable infusion pump, and catheters were removed on the fourth postoperative day.
Results: Patients given 4 days of perineural ropivacaine (n = 24) attained all three discharge criteria in a median (25th-75th percentiles) of 29 (24-45) h, compared with 51 (42-73) h for those of the control group (n = 23; estimated ratio = 0.62; 95% confidence interval, 0.45-0.92; P = 0.011). Patients assigned to receive ropivacaine ambulated a median of 34 (9-55) m the afternoon after surgery, compared with 20 (6-46) m for those receiving normal saline (estimated ratio = 1.3; 95% confidence interval, 0.6-3.0; P = 0.42). Three falls occurred in subjects receiving ropivacaine (13%), versus none in subjects receiving normal saline.
Conclusions: Compared with an overnight cLPB, a 4-day ambulatory cLPB decreases the time to reach three predefined discharge criteria by an estimated 38% after hip arthroplasty. However, the extended infusion did not increase ambulation distance to a statistically significant degree.
Figures
References
-
- Anderson FA, Jr, Hirsh J, White K, Fitzgerald RH., Jr Temporal trends in prevention of venous thromboembolism following primary total hip or knee arthroplasty 1996-2001: Findings from the Hip and Knee Registry. Chest. 2003;124:349S–56S. - PubMed
-
- Roberts GW, Bekker TB, Carlsen HH, Moffatt CH, Slattery PJ, McClure AF. Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth Analg. 2005;101:1343–8. - PubMed
-
- Matheny JM, Hanks GA, Rung GW, Blanda JB, Kalenak A. A comparison of patient-controlled analgesia and continuous lumbar plexus block after anterior cruciate ligament reconstruction. Arthroscopy. 1993;9:87–90. - PubMed
-
- Strassels SA, Chen C, Carr DB. Postoperative analgesia: Economics, resource use, and patient satisfaction in an urban teaching hospital. Anesth Analg. 2002;94:130–7. - PubMed
-
- Leali A, Fetto J, Moroz A. Prevention of thromboembolic disease after non-cemented hip arthroplasty: A multimodal approach. Acta Orthop Belg. 2002;68:128–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
