

Case Reports
doi: 10.1590/s1807-59322008000400026.
A case of pseudo-hypertrophic cardiomyopathy: a congenital heart disease
- PMID: 18719773
- PMCID: PMC2664138
- DOI: 10.1590/s1807-59322008000400026
Item in Clipboard
Case Reports
A case of pseudo-hypertrophic cardiomyopathy: a congenital heart disease
Clinics (Sao Paulo).
2008 Aug.
No abstract available
Figures
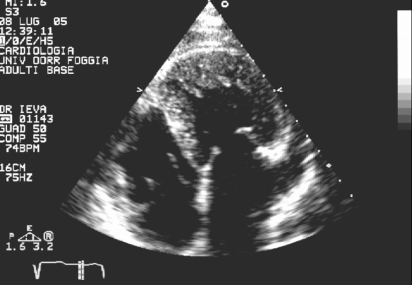
Detail of the three-leaflet tricuspid valve
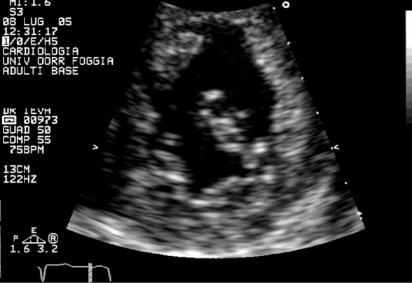
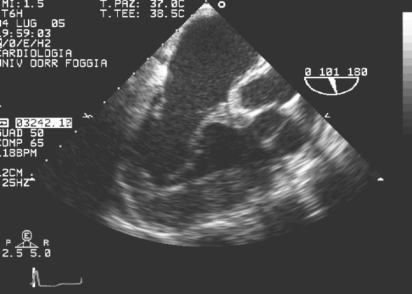
Apical four-chamber view shows dilatation of both the left atrium and left appendage and a smooth interventricular septalright surface against the trabeculated septal left surface in the correct position (normal atrial situs). This permits diagnosis of ventricular inversion and the presence of a three-leaflet tricuspid valve inserted more apically than the mitral valve
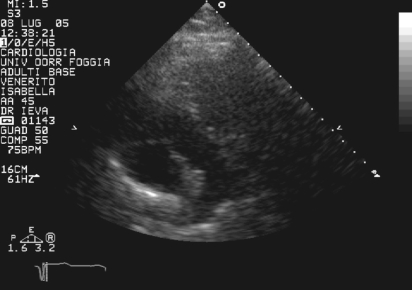
The pulmonary trunk, identified by its bifurcation
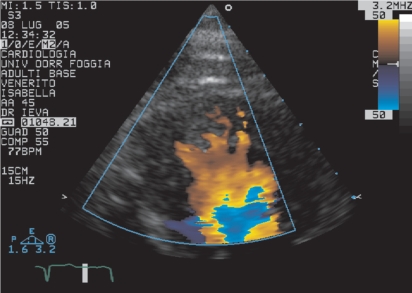
Details of the systemic ventricle apical segments with prominent trabeculations and color flow imaging. This analysis reveals forward and reverse flow between trabeculae during the cardiac cycle

Transesophageal examination shows the morphological features of the appendage
In prominent systemic ventricle hypertrophy, the aortic valve and the systemic atrioventricular valve are discontinuous because of muscle interposition
Similar articles
-
Membranous subaortic stenosis coexisting with hypertrophic cardiomyopathy: A case report.J Clin Ultrasound. 2018 Nov;46(9):610-613. doi: 10.1002/jcu.22613. Epub 2018 Sep 19. J Clin Ultrasound. 2018. PMID: 30229919
-
Left ventricular non-compaction associated with hypertrophic cardiomyopathy in the same patient.Kardiol Pol. 2017;75(4):397. doi: 10.5603/KP.2017.0064. Kardiol Pol. 2017. PMID: 28421585 No abstract available.
-
Echocardiographic comparison between left ventricular non-compaction and hypertrophic cardiomyopathy.Int J Cardiol. 2017 Feb 1;228:900-905. doi: 10.1016/j.ijcard.2016.11.162. Epub 2016 Nov 9. Int J Cardiol. 2017. PMID: 27894062
-
Echocardiography in hypertrophic cardiomyopathy: the role of conventional and emerging technologies.JACC Cardiovasc Imaging. 2008 Nov;1(6):787-800. doi: 10.1016/j.jcmg.2008.09.002. Epub 2008 Nov 18. JACC Cardiovasc Imaging. 2008. PMID: 19356516 Review.
-
[Ultrasonic diagnosis of congenital heart defects].Kardiologiia. 1977 Jan;17(1):139-46. Kardiologiia. 1977. PMID: 323552 Review. Russian. No abstract available.
Cited by
-
Anti-hypertensive drugs have different effects on ventricular hypertrophy regression.Clinics (Sao Paulo). 2010 Jul;65(7):723-8. doi: 10.1590/S1807-59322010000700012. Clinics (Sao Paulo). 2010. PMID: 20668631 Free PMC article. Review.
References
-
- Von Rokitansky K. Pathologisch-anatomische Abhandlung. Vienna: W. Braumuller; 1875. pp. 83–6.
-
- Warnes CA. Transposition of the great arteries. Circulation. 2006;12(114):2699–709. - PubMed
-
- Ikeda U, Furuse M, Suzuki O, Kimura K, Sekiguchi H, Shimada K. Long term survival in aged patients with corrected transposition of the great arteries. Chest. 1992;101:1382–5. - PubMed
-
- Graham TP, Jr, Bernard YD, Mellen BG, Celermajer D, Baumgartner H, Cetta F, et al. Long-term outcome in congenitally corrected transposition of the great arteries: a multi-institutional study. J Am Coll Cardiol. 2000;36:255–61. - PubMed
-
- Lundstrom U, Bull C, Wyse RKH, Somerville J. The natural and “unnatural” history of congenitally corrected transposition. Am J Cardiol. 1990;65:1222–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
