

Results of the hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone regimen in elderly patients with acute lymphocytic leukemia
- PMID: 18720356
- PMCID: PMC4199453
- DOI: 10.1002/cncr.23819
Results of the hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone regimen in elderly patients with acute lymphocytic leukemia
Abstract
Background: Understanding the causes of failure in older patients with acute lymphocytic leukemia (ALL) may help improve treatment strategies for patients in this particular age group.
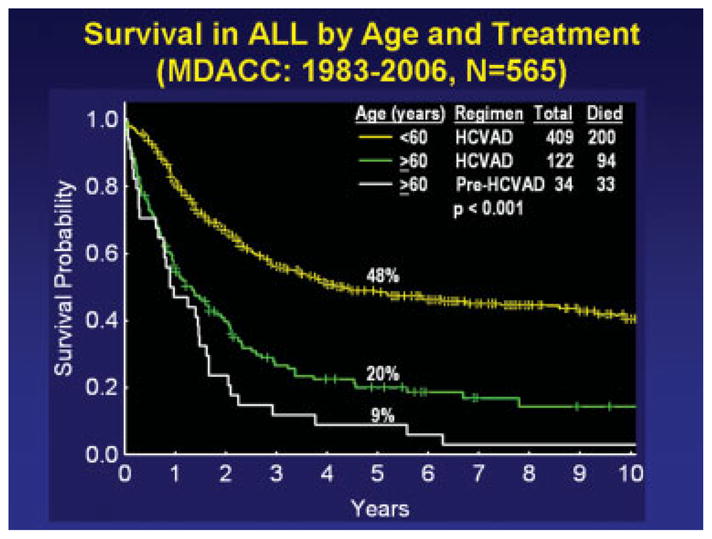
Methods: The objectives of the current study were to define the causes of death in older patients (aged > or = 60 years) with ALL during induction and consolidation-maintenance with a dose-intensive regimen of alternating 8 courses of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD) with high doses of methotrexate and cytarabine followed by maintenance with 6-mercaptopurine, vincristine, methotrexate, and prednisone and to compare their outcomes with the outcomes of older patients who received earlier, less intensive regimens and younger patients who received hyper-CVAD. One hundred twenty-two older patients who received hyper-CVAD were compared with 34 older patients who received less intensive regimens and with 409 younger patients who received hyper-CVAD.
Results: The complete response (CR) rates in older patients receiving hyper-CVAD, older patients receiving other regimens, and younger patients receiving hyper-CVAD were 84%, 59%, and 92%, respectively (P < .001); and the respective induction mortality rates were 10%, 12%, and 2% (P not significant in older patients). The incidence of disease resistance during induction was 5%, 27%, and 2%, respectively (P < .001). The majority of deaths were related to infections. Among patients who achieved a CR, death in CR was noted in 34%, 15%, and 7% of older patients receiving hyper-CVAD, older patients receiving other regimens, and younger patients, respectively (P < .001); and the respective rates of recurrence were 40%, 80%, and 48% (P = .004). The estimated 5-year survival rates were 20%, 9%, and 48%, respectively (P < .001).
Conclusions: The results of the current study suggested that intensifying the chemotherapy in older patients with ALL reduced the incidence of leukemia resistance but increased the incidence of death in CR from myelosuppression-associated infections. The overall benefit:risk ratio was favorable. Identifying novel, low-intensity agents/regimens for older patients with ALL may improve the results further.
(c) 2008 American Cancer Society.
Figures
References
-
- Pui CH, Evans WE. Acute lymphoblastic leukemia. N Engl J Med. 1998;339:605–615. - PubMed
-
- Schrappe M, Reiter A, Ludwig WD, et al. Improved outcome in childhood acute lymphoblastic leukemia despite reduced use of anthracyclines and cranial radiotherapy: results of trial ALL-BFM 90. German-Austrian-Swiss ALL-BFM Study Group. Blood. 2000;95:3310–3322. - PubMed
-
- Silverman LB, Gelber RD, Dalton VK, et al. Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood. 2001;97:1211–1218. - PubMed
-
- Nachman JB, Sather HN, Sensel MG, et al. Augmented post-induction therapy for children with high-risk acute lymphoblastic leukemia and a slow response to initial therapy. N Engl J Med. 1998;338:1663–1671. - PubMed
-
- Kantarjian H, Thomas D, O’Brien S, et al. Long-term follow-up results of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD), a dose-intensive regimen, in adult acute lymphocytic leukemia. Cancer. 2004;101:2788–2801. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
