

Changing trends of hospital utilization in patients after their first episode of atrial fibrillation
- PMID: 18721513
- PMCID: PMC3743254
- DOI: 10.1016/j.amjcard.2008.04.025
Changing trends of hospital utilization in patients after their first episode of atrial fibrillation
Abstract
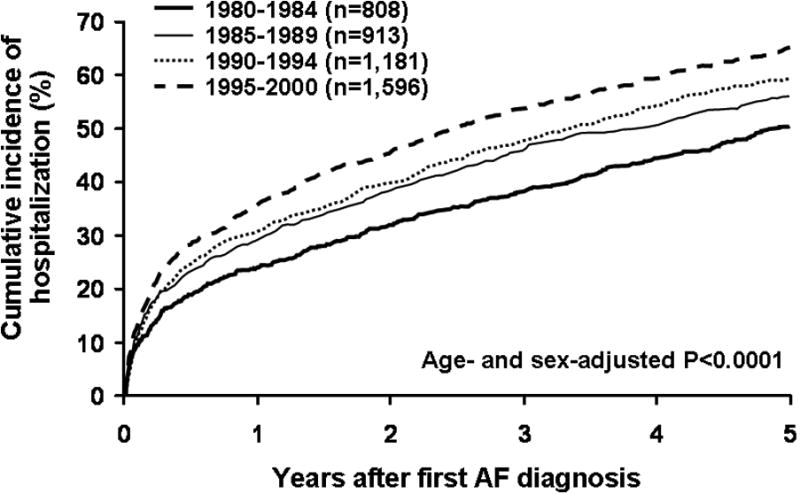
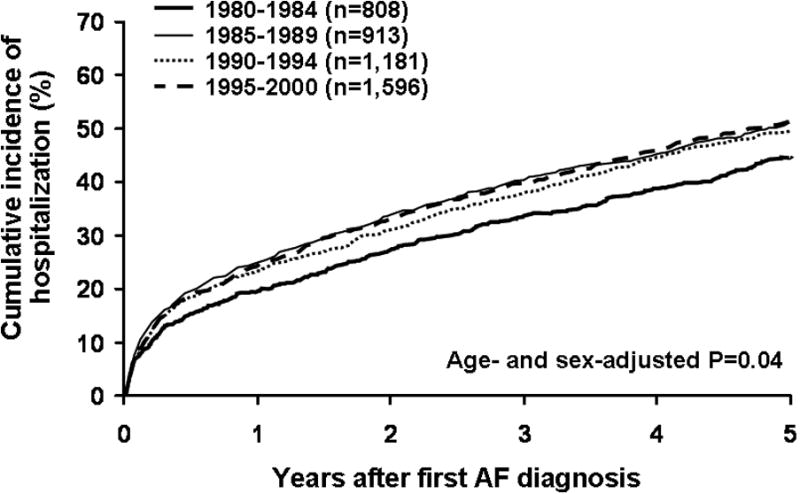
A marked increase in hospitalization for patients with atrial fibrillation (AF) has previously been noted. Whether this increase is related to a change in the prevalence of AF or a change in the pattern of practice with respect to the management of AF remains unclear. To determine the trends in hospital utilization after first AF in a community-based setting (Olmsted County, Minnesota), residents diagnosed with first AF from 1980 to 2000 were identified and followed until 2004. The primary outcome of interest was hospital admission for cardiovascular reasons. Of a total of 4,498 subjects (73 +/- 14 years old, 51% men), 2,503 (56%) were admitted to the hospital for cardiovascular causes >or=1 time during a mean follow-up of 5.5 +/- 5.0 years. Risk of first hospitalization was greatest during the first year of AF (cumulative incidence 31%, 95% confidence interval [CI] 30 to 32). First hospitalization was strongly related to age (p <0.0001) but not to sex (p = 0.38). From 1980 to 2000, the age-and sex-adjusted rate of first hospitalization increased, on average, by 2.5% a year (95% CI 1.8 to 3.2, p <0.0001), even after multivariable adjustment for co-morbidities. When we excluded all hospital admissions for the purposes of AF management, the increase in hospitalization was only 0.8% per year (95% CI 0.05 to 1.6, p = 0.04), which was no longer significant after multivariable adjustment for co-morbidities (p = 0.25). In conclusion, the marked increase in hospitalization after first AF diagnosis from 1980 to 2000 appeared to be largely driven by the changing practice pattern in AF management.
Conflict of interest statement
There are no conflicts of interest on the part of any authors.
Figures
References
-
- Wattigney WA, Mensah GA, Croft JB. Increasing trends in hospitalization for atrial fibrillation in the United States, 1985 through 1999: implications for primary prevention. Circulation. 2003;108:711–716. - PubMed
-
- Humphries KH, Jackevicius C, Gong Y, Svensen L, Cox J, Tu JV, Laupacis A. Population rates of hospitalization for atrial fibrillation/flutter in Canada. Can J Cardiol. 2004;20:869–876. - PubMed
-
- Friberg J, Buch P, Scharling H, Gadsbphioll N, Jensen GB. Rising rates of hospital admissions for atrial fibrillation. Epidemiology. 2003;14:666–672. - PubMed
-
- Stewart S, MacIntyre K, MacLeod MM, Bailey AE, Capewell S, McMurray JJ. Trends in hospital activity, morbidity and case fatality related to atrial fibrillation in Scotland, 1986-1996. Eur Heart J. 2001;22:693–701. - PubMed
-
- Frost L, Engholm G, Moller H, Husted Decrease in mortality in patients with a hospital diagnosis of atrial fibrillation in Denmark during the period 1980-1993. Eur Heart J. 1999;20:1592–1599. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
