

Ventricular function deteriorates with recurrent coarctation in hypoplastic left heart syndrome
- PMID: 18721575
- PMCID: PMC11227908
- DOI: 10.1016/j.athoracsur.2008.04.074
Ventricular function deteriorates with recurrent coarctation in hypoplastic left heart syndrome
Abstract
Background: Recurrent coarctation (re-CoA) after stage I palliation in hypoplastic left heart syndrome (HLHS) is deleterious. We studied whether re-CoA had an effect on ventricular systolic function.
Methods: Retrospectively reviewed were HLHS patients surviving stage I Norwood palliation (stage I) and cavopulmonary shunt (CPS) between January 2004 and February 2007. Echocardiographic right ventricular fractional area change (RV-FAC) was used to evaluate ventricular systolic function after stage I, before CPS, and before Fontan procedures. Cardiac catheterization and magnetic resonance imaging data before CPS were reviewed to assess re-CoA, using a coarctation index (CI = isthmus diameter/descending aortic diameter).
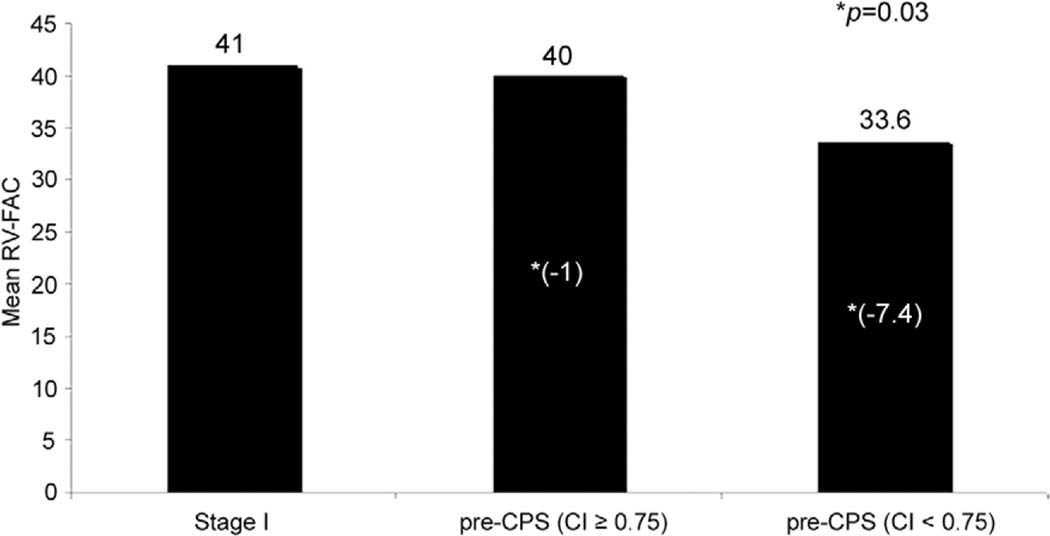
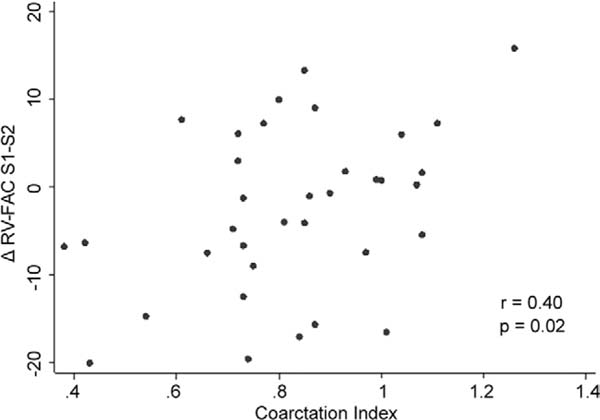
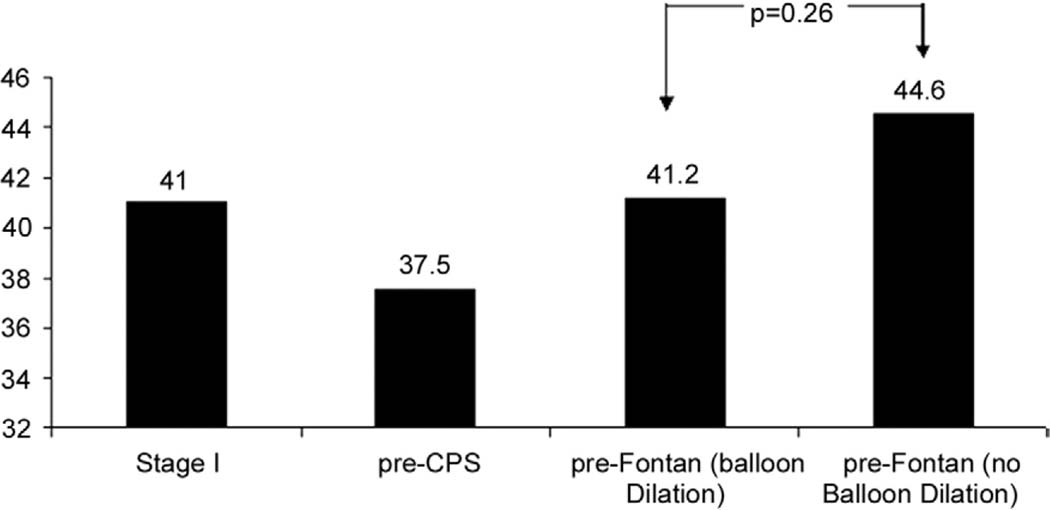
Results: Fifty-one patients were included, and 21 had a CI of less than 0.75 (mean, 0.82 +/- 0.19; 21). Twelve patients required arch balloon dilation between CPS and Fontan. The change of RV-FAC for all patients between stage I and CPS was -2.2% +/- 9.6%. Pearson correlation coefficient demonstrated a significant correlation between lower CI values and lower RV-FAC at the pre-CPS echocardiogram (r = .35, p = 0.03); and lower CI values and greater decrease in RV-FAC between stage I and pre-CPS evaluation (r = 0.40, p = 0.018). At follow-up pre-Fontan, RV-FAC for patients who underwent balloon dilation for re-CoA recovered to a level that was inferior but not significantly different from that of patients who did not need balloon dilation.
Conclusions: Recurrent aortic arch obstruction after stage I for HLHS is associated with worse RV systolic function at the time of stage II operation. Timely intervention on the re-CoA results in recovery of RV function.
Figures
References
-
- Bautista-Hernandez V, Marx GR, Gauvreau K, et al. Coarctectomy reduces neoaortic arch obstruction in Hypoplastic left heart syndrome. J Thorac Cardiovasc Surg 2007;133: 1540–6. - PubMed
-
- Tworetzky W, McElhinney DB, Burch GH, Teitel DF, Moore P. Balloon arterioplasty of recurrent coarctation after the modified Norwood procedure in infants. Catheter Cardiovasc Interv 2000;50:54–8. - PubMed
-
- Burkhart HM, Ashburn DA, Konstantinov IE, et al. Interdigitating arch reconstruction eliminates recurrent coarctation after the Norwood procedure. J Thorac Cardiovasc Surg 2005;130:61–5. - PubMed
-
- Chessa M, Dindar A, Vettukattil JJ, et al. Balloon angioplasty in infants with aortic obstruction after the modified stage I Norwood procedure. Am Heart J 2000;140:227–31. - PubMed
-
- Fraisse A, Colan SD, Jonas RA, Gauvreau K, Geva T. Accuracy of echocardiography for detection of aortic arch obstruction after stage I Norwood procedure. Am Heart J 1998;135:230–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
