

Four-dimensional computed tomography-based treatment planning for intensity-modulated radiation therapy and proton therapy for distal esophageal cancer
- PMID: 18722278
- PMCID: PMC2610812
- DOI: 10.1016/j.ijrobp.2008.05.014
Four-dimensional computed tomography-based treatment planning for intensity-modulated radiation therapy and proton therapy for distal esophageal cancer
Abstract
Purpose: To compare three-dimensional (3D) and four-dimensional (4D) computed tomography (CT)-based treatment plans for proton therapy or intensity-modulated radiation therapy (IMRT) for esophageal cancer in terms of doses to the lung, heart, and spinal cord and variations in target coverage and normal tissue sparing.
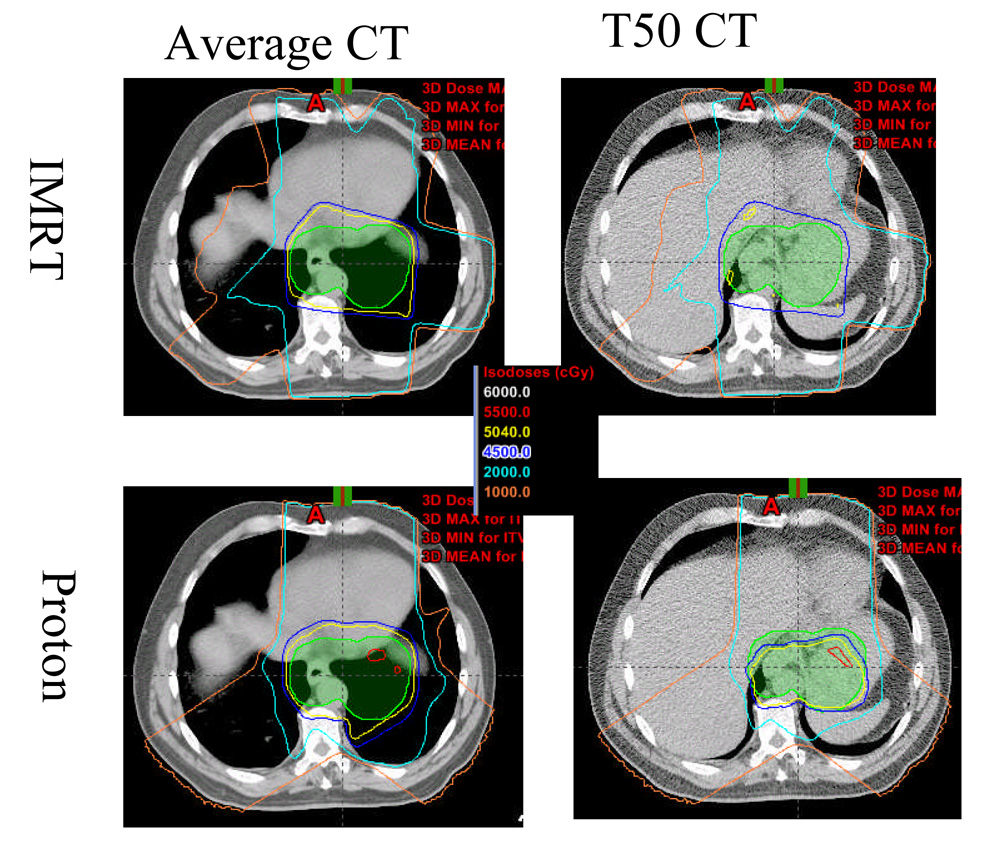
Methods and materials: The IMRT and proton plans for 15 patients with distal esophageal cancer were designed from the 3D average CT scans and then recalculated on 10 4D CT data sets. Dosimetric data were compared for tumor coverage and normal tissue sparing.
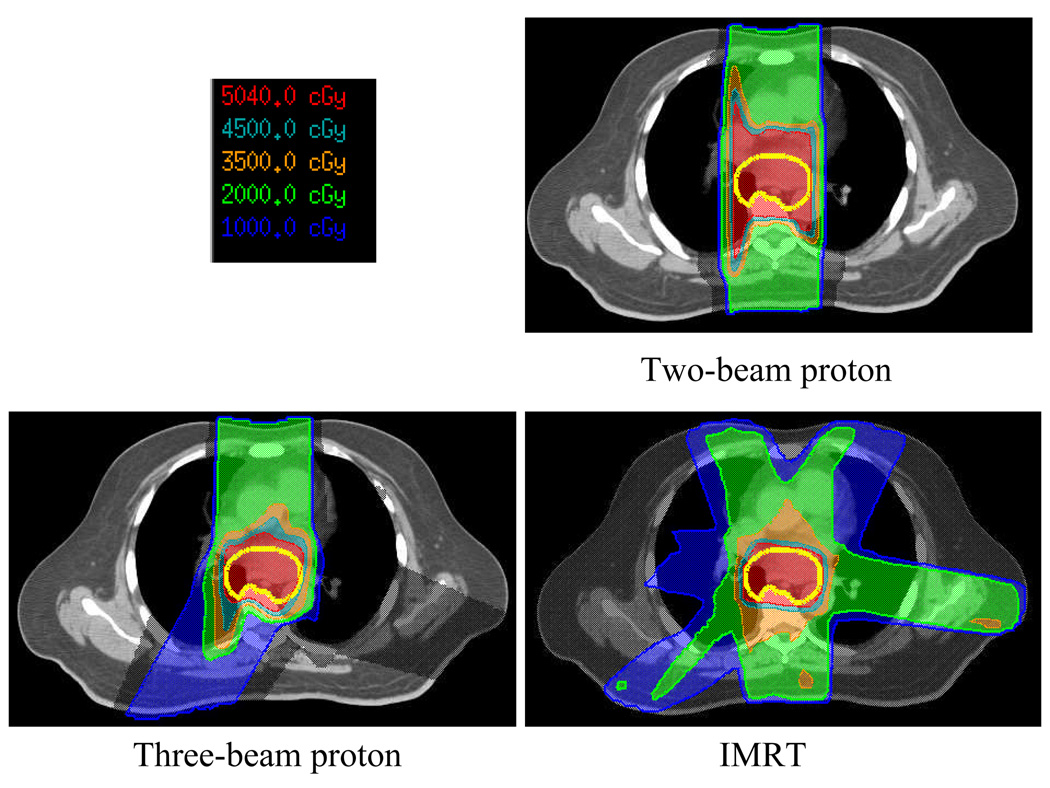
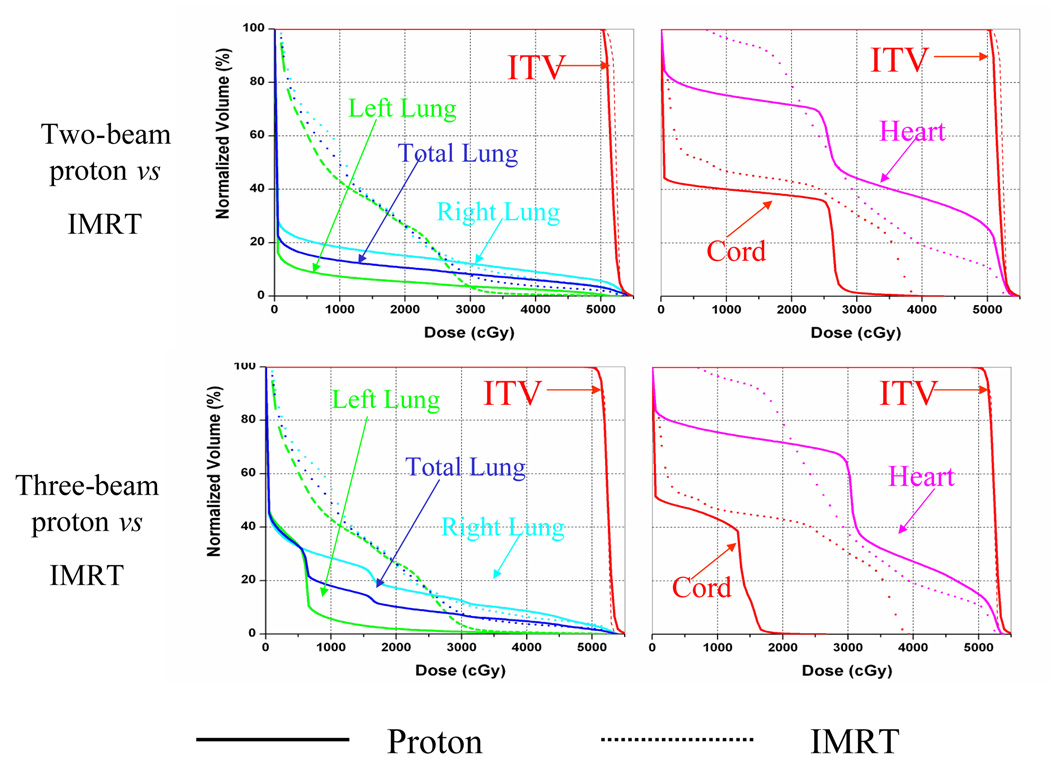
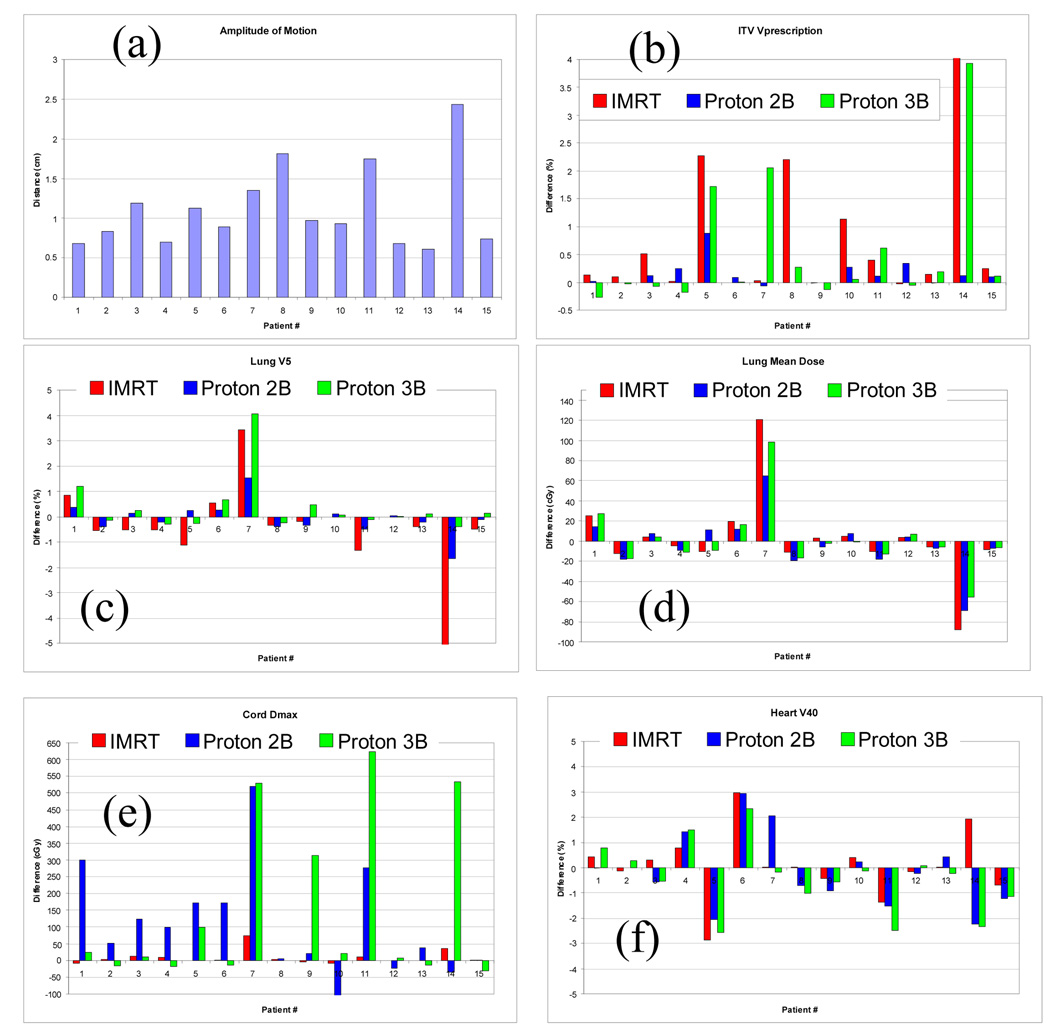
Results: Compared with IMRT, median lung volumes exposed to 5, 10, and 20 Gy and mean lung dose were reduced by 35.6%, 20.5%, 5.8%, and 5.1 Gy for a two-beam proton plan and by 17.4%, 8.4%, 5%, and 2.9 Gy for a three-beam proton plan. The greater lung sparing in the two-beam proton plan was achieved at the expense of less conformity to the target (conformity index [CI], 1.99) and greater irradiation of the heart (heart-V40, 41.8%) compared with the IMRT plan(CI, 1.55, heart-V40, 35.7%) or the three-beam proton plan (CI, 1.46, heart-V40, 27.7%). Target coverage differed by more than 2% between the 3D and 4D plans for patients with substantial diaphragm motion in the three-beam proton and IMRT plans. The difference in spinal cord maximum dose between 3D and 4D plans could exceed 5 Gy for the proton plans partly owing to variations in stomach gas filling.
Conclusions: Proton therapy provided significantly better sparing of lung than did IMRT. Diaphragm motion and stomach gas-filling must be considered in evaluating target coverage and cord doses.
Conflict of interest statement
Conflict Interest: None
Figures

References
-
- Lin FCF, Durkin AE, Ferguson MK. Induction therapy does not increase surgical morbidity after esophagectomy for cancer. Annals of Thoracic Surgery. 2004;78:1783–1789. - PubMed
-
- Lee HK, Vaporciyan AA, Cox JD, et al. Postoperative pulmonary complications after preoperative chemoradiation for esophageal carcinoma: Correlation with pulmonary dose-volume histogram parameters. International Journal of Radiation Oncology Biology Physics. 2003;57:1317–1322. - PubMed
-
- Wang SL, Liao ZX, Vaporciyan AA, et al. Investigation of clinical and dosimetric factors associated with postoperative pulmonary complications in esophageal cancer patients treated with concurrent chemoradiotherapy followed by surgery. International Journal of Radiation Oncology Biology Physics. 2006;64:692–699. - PubMed
-
- Guerrero T, Castillo R, Noyola-Martinez J, et al. Reduction of pulmonary compliance found with high-resolution computed tomography in irradiated mice. International Journal of Radiation Oncology Biology Physics. 2007;67:879–887. - PubMed
