

Immunosuppressive therapy mitigates immunological rejection of human embryonic stem cell xenografts
- PMID: 18728188
- PMCID: PMC2529073
- DOI: 10.1073/pnas.0805802105
Immunosuppressive therapy mitigates immunological rejection of human embryonic stem cell xenografts
Abstract
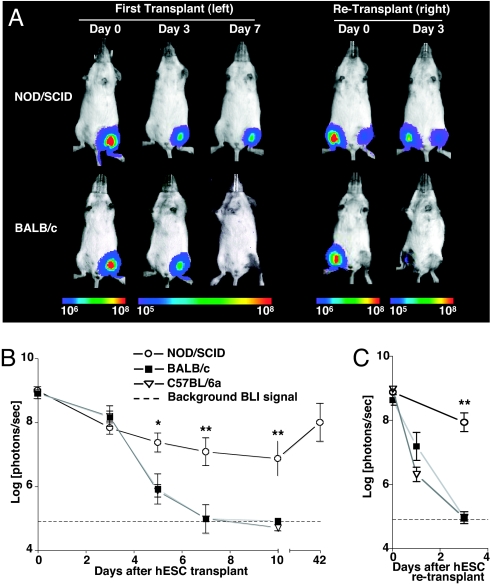
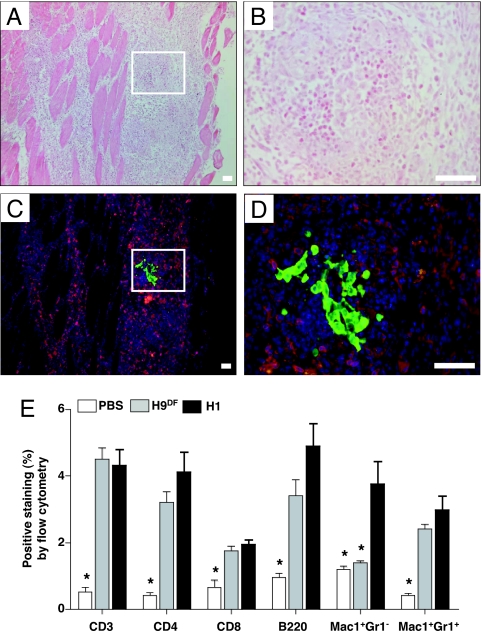
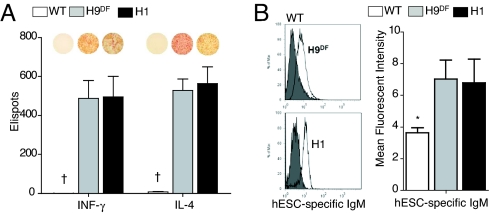
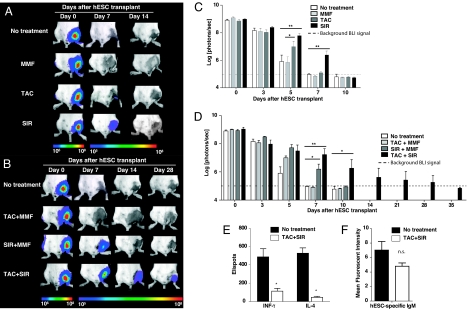
Given their self-renewing and pluripotent capabilities, human embryonic stem cells (hESCs) are well poised as a cellular source for tissue regeneration therapy. However, the host immune response against transplanted hESCs is not well characterized. In fact, controversy remains as to whether hESCs have immune-privileged properties. To address this issue, we used in vivo bioluminescent imaging to track the fate of transplanted hESCs stably transduced with a double-fusion reporter gene consisting of firefly luciferase and enhanced GFP. We show that survival after transplant is significantly limited in immunocompetent as opposed to immunodeficient mice. Repeated transplantation of hESCs into immunocompetent hosts results in accelerated hESC death, suggesting an adaptive donor-specific immune response. Our data demonstrate that transplanted hESCs trigger robust cellular and humoral immune responses, resulting in intragraft infiltration of inflammatory cells and subsequent hESC rejection. Moreover, we have found CD4(+) T cells to be an important modulator of hESC immune-mediated rejection. Finally, we show that immunosuppressive drug regimens can mitigate the anti-hESC immune response and that a regimen of combined tacrolimus and sirolimus therapies significantly prolongs survival of hESCs for up to 28 days. Taken together, these data suggest that hESCs are immunogenic, trigger both cellular and humoral-mediated pathways, and, as a result, are rapidly rejected in xenogeneic hosts. This process can be mitigated by a combined immunosuppressive regimen as assessed by molecular imaging approaches.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Thomson JA, et al. Embryonic stem cell lines derived from human blastocysts. Science. 1998;282:1145–1147. - PubMed
-
- Laflamme MA, et al. Cardiomyocytes derived from human embryonic stem cells in pro-survival factors enhance function of infarcted rat hearts. Nat Biotechnol. 2007;25:1015–1024. - PubMed
-
- Ben-Hur T, et al. Transplantation of human embryonic stem cell-derived neural progenitors improves behavioral deficit in Parkinsonian rats. Stem Cells. 2004;22:1246–1255. - PubMed
-
- Swijnenburg RJ, van der Bogt KE, Sheikh AY, Cao F, Wu JC. Clinical hurdles for the transplantation of cardiomyocytes derived from human embryonic stem cells: Role of molecular imaging. Curr Opin Biotechnol. 2007;18:38–45. - PubMed
-
- Bradley JA, Bolton EM, Pedersen RA. Stem cell medicine encounters the immune system. Nat Rev Immunol. 2002;2:859–871. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
