

Proportional classifications of COPD phenotypes
- PMID: 18728201
- PMCID: PMC2862964
- DOI: 10.1136/thx.2007.089193
Proportional classifications of COPD phenotypes
Erratum in
- Thorax. 2014 Jul;69(7):672
-
Correction.Thorax. 2015 Sep;70(9):905. doi: 10.1136/thx.2007.089193corr2. Thorax. 2015. PMID: 26272930 No abstract available.
Abstract
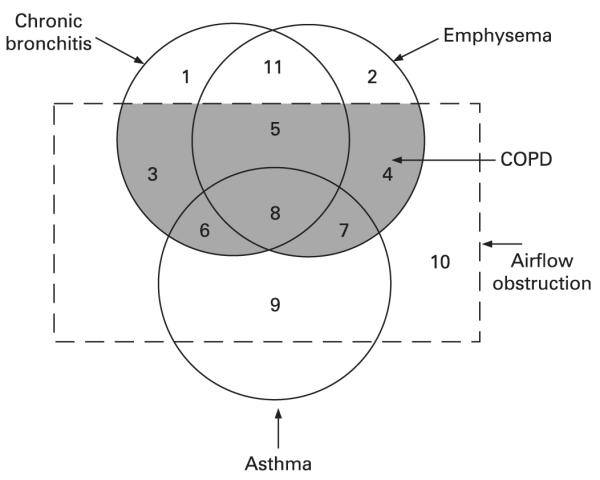
Background: Chronic obstructive pulmonary disease (COPD) encompasses a group of disorders characterised by the presence of incompletely reversible airflow obstruction with overlapping subsets of different phenotypes including chronic bronchitis, emphysema or asthma. The aim of this study was to determine the proportion of adult subjects aged >50 years within each phenotypic subgroup of COPD, defined as a post-bronchodilator ratio of forced expiratory volume in 1 s/forced vital capacity (FEV(1)/FVC) <0.7, in accordance with current international guidelines.
Methods: Adults aged >50 years derived from a random population-based survey undertook detailed questionnaires, pulmonary function tests and chest CT scans. The proportion of subjects in each of 16 distinct phenotypes was determined based on combinations of chronic bronchitis, emphysema and asthma, with and without incompletely reversible airflow obstruction defined by a post-bronchodilator FEV(1)/FVC ratio of 0.7.
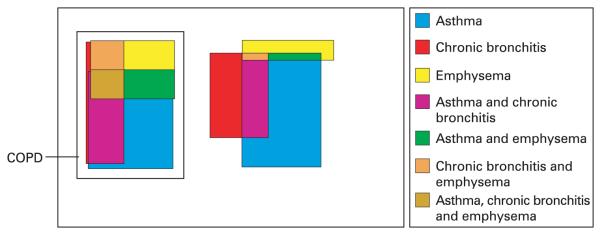
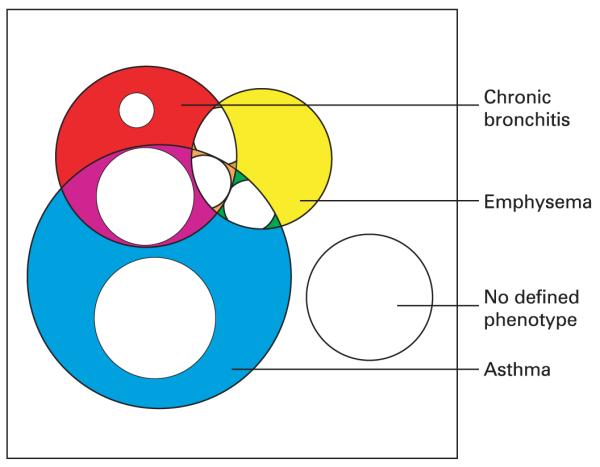
Results: A total of 469 subjects completed the investigative modules, 96 of whom (20.5%) had COPD. Diagrams were constructed to demonstrate the relative proportions of the phenotypic subgroups in subjects with and without COPD. 18/96 subjects with COPD (19%) had the classical phenotypes of chronic bronchitis and/or emphysema but no asthma; asthma was the predominant COPD phenotype, being present in 53/96 (55%). When COPD was defined as a post-bronchodilator FEV(1)/FVC less than the lower limit of normal, there were one-third fewer subjects with COPD and a smaller proportion without a defined emphysema, chronic bronchitis or asthma phenotype.
Conclusion: This study provides proportional classifications of the phenotypic subgroups of COPD which can be used as the basis for further research into the pathogenesis and treatment of this heterogeneous disorder.
Figures
Comment in
-
COPD, diagrams and traditions: time to move on?Thorax. 2008 Sep;63(9):755-6. doi: 10.1136/thx.2007.092924. Thorax. 2008. PMID: 18728198 No abstract available.
References
-
- Mannino DM, Watt G, Hole D, et al. The natural history of chronic obstructive pulmonary disease. Eur Respir J. 2006;27:627–43. - PubMed
-
- Anon. Terminology, definitions, and classification of chronic pulmonary emphysema and related conditions. A report of the conclusions of a Ciba guest symposium. Thorax. 1959;14:286–99.
-
- Snider G. Chronic obstructive pulmonary disease: a definition and implications of structural determinants of airflow obstruction for epidemiology. Am Rev Respir Dis. 1989;140(3 Pt 2):S3–8. - PubMed
-
- American Thoracic Society Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1995;152(5 Pt 2):S77–121. - PubMed
-
- Celli B, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23:932–46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical