

Developments in the management of autosomal dominant polycystic kidney disease
- PMID: 18728845
- PMCID: PMC2504069
- DOI: 10.2147/tcrm.s1617
Developments in the management of autosomal dominant polycystic kidney disease
Abstract
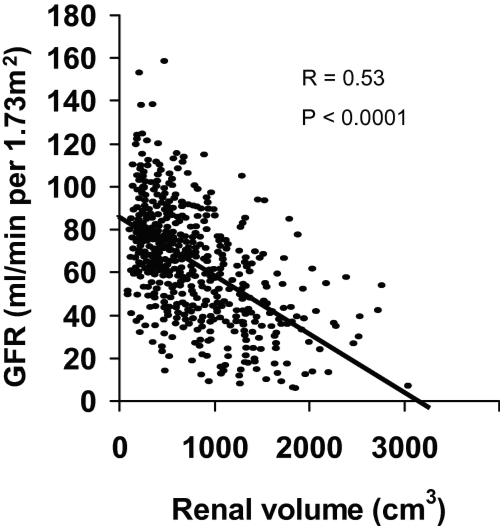
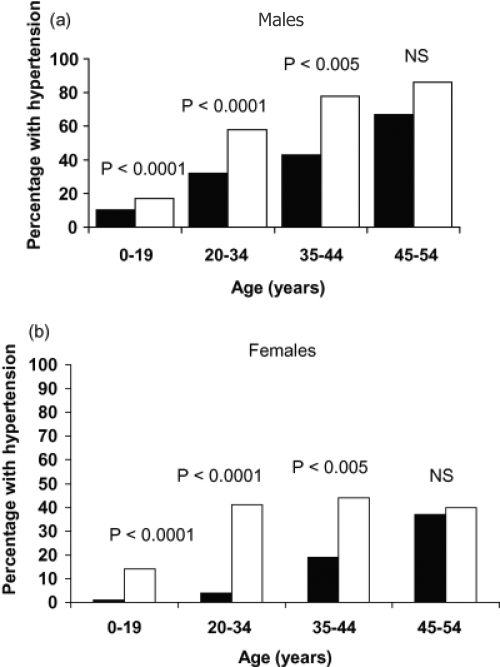
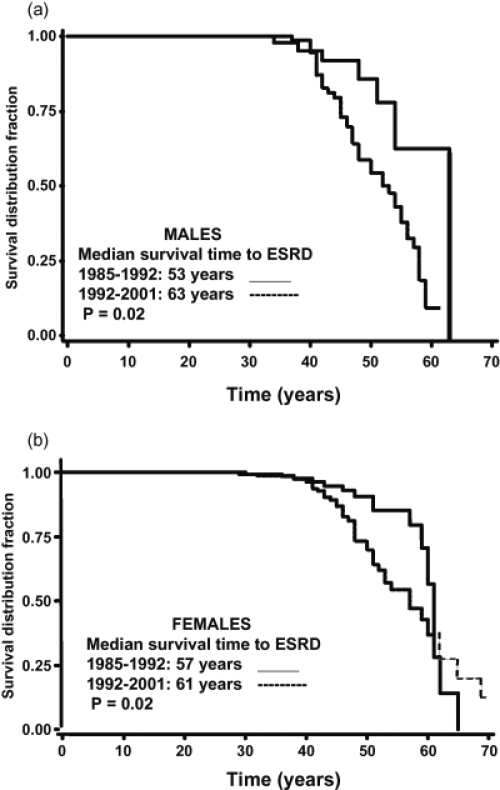
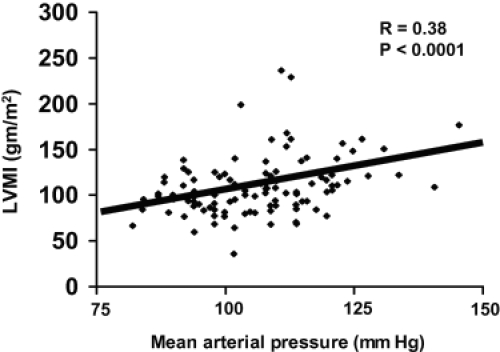
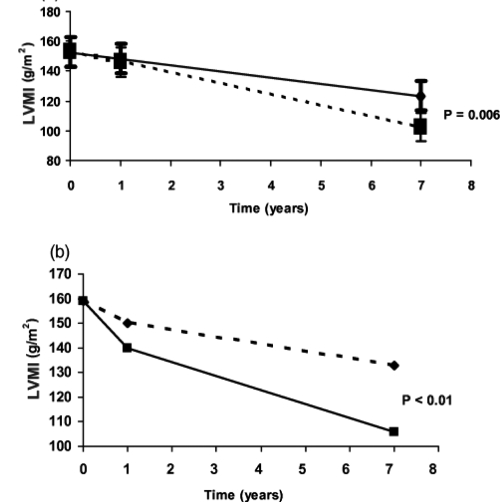
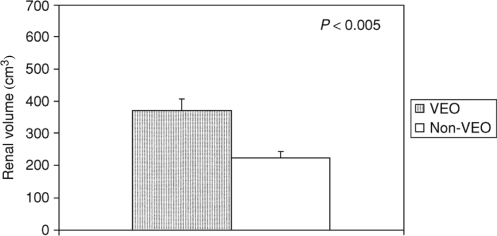
Autosomal dominant polycystic kidney disease (ADPKD) is the most frequent life- threatening, hereditary disease. ADPKD is more common than sickle cell anemia, cystic fibrosis, muscular dystrophy, hemophilia, Down's syndrome, and Huntington's disease combined. ADPKD is a multisystemic disorder characterized by the progressive development of renal cysts and marked renal enlargement. Structural and functional renal deterioration occurs in ADPKD patients and is the fourth leading cause of end-stage renal disease (ESRD) in adults. Aside from the renal manifestations, extrarenal structural abnormalities, such as liver cysts, cardiovascular abnormalities, and intracranial aneurysms may lead to morbidity and mortality. Recent studies have identified prognostic factors for progressive renal impairment including gender, race, age, proteinuria, hematuria, hypertension and increased left ventricular mass index (LVMI). Early diagnosis and better understanding of the pathophysiology of the disease provides the opportunity to aggressivly treat hypertension with renin-angiotensin-aldosterone system inhibitors and thereby potentially reduce LVMI, prevent cardiovascular morbidity and mortality and slow progression of the renal disease.
Keywords: cerebral aneurysms; hypertension; left ventricular hypertrophy; liver cysts; renal pain.
Figures
References
-
- Anderson RJ, Miller PD, Linas SL, et al. Role of the renin-angiotensin system in hypertension of polycystic kidney disease. Mineral Electrolyte Metab. 1979;2:137–41.
-
- Anderson GA, Degroot D, Lawson RK. Polycystic renal disease. Urol. 1993;42:358–64. - PubMed
-
- Bajwa ZH, Gupta S, Warfield CA, et al. Pain management in polycystic kidney disease. Kidney Int. 2001;60:1631–44. - PubMed
-
- Bajwa ZH, Sial KA, Malik AB, et al. Pain patterns in patients with polycystic kidney disease. Kidney Int. 2004;66:1561–9. - PubMed
-
- Bardaji A, Matinez-Vea A, Gutierrez C, et al. Left ventricular mass and diastolic function in normotensive young adults with autosomal dominant polycystic kidney disease. Am J Kidney Dis. 1998;32:970–5. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
