

Early experiences of robotic-assisted laparoscopic liver resection
- PMID: 18729307
- PMCID: PMC2615291
- DOI: 10.3349/ymj.2008.49.4.632
Early experiences of robotic-assisted laparoscopic liver resection
Abstract
Purpose: The surgical robotic system is superior to traditional laparoscopy in regards to 3-dimensional images and better instrumentations. Robotic surgery for hepatic resection has not yet been extensively reported.
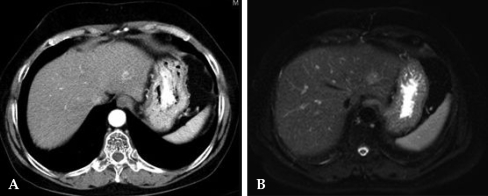
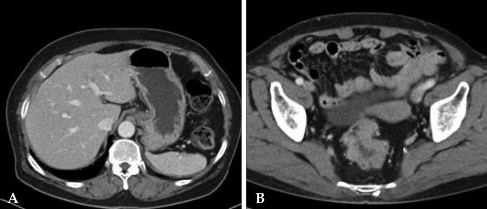
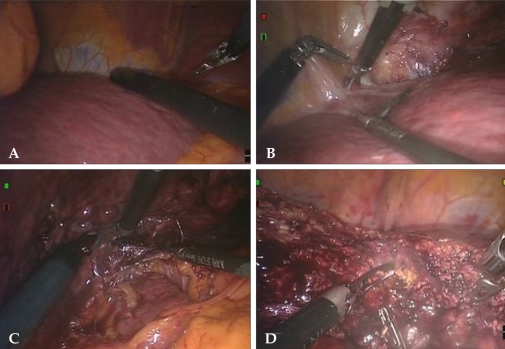
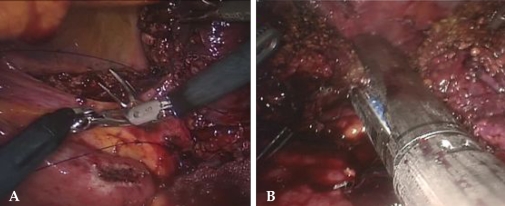
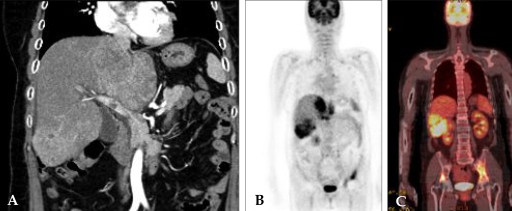
Patients and methods: Between March and May 2007, we performed 3 robot-assisted left lateral sectionectomies of the liver. Case 1 had a hepatocellular carcinoma (HCC), case 2 had colon cancer with liver metastasis, and case 3 had intrahepatic duct stones.
Results: All patients had successful operation and recovered without complications. Shorter length of hospital stays, earlier start of oral feeding and less amount of ascites were found. However, case 1 had recurrent HCC at 3 months after operation.
Conclusion: Robotic-assisted liver surgery is still a new field in its developing stage. In patients with small malignant tumors and benign liver diseases, robotic-assisted laparoscopic resection is feasible and safe. Through experience, the use of robotics is expected to increase in the treatment of benign diseases and malignant neoplasms. However, careful patient selection is important and long-term outcomes need to be evaluated.
Figures

References
-
- Hanly EJ, Talamini MA. Robotic abdominal surgery. Am J Surg. 2004;188(4A Suppl):19S–26S. - PubMed
-
- Vidovszky TJ, Smith W, Ghosh J, Ali MR. Robotic cholecystectomy: learning curve, advantages, and limitations. J Surg Res. 2006;136:172–178. - PubMed
-
- Hashizume M, Tsugawa K. Robotic surgery and cancer: the present state, problems and future vision. Jpn J Clin Oncol. 2004;34:227–237. - PubMed
-
- D'Annibale A, Morpurgo E, Fiscon V, Trevisan P, Sovernigo G, Orsini C, et al. Robotic and laparoscopic surgery for treatment of colorectal disease. Dis Colon Rectum. 2004;47:2162–2168. - PubMed
-
- Camarillo DB, Krummel TM, Salisbury JK., Jr Robotic technology in surgery: past, present, and future. Am J Surg. 2004;188(4A Suppl):2S–15S. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
