

The mechanics of external fixation
- PMID: 18751766
- PMCID: PMC2504087
- DOI: 10.1007/s11420-006-9025-0
The mechanics of external fixation
Abstract
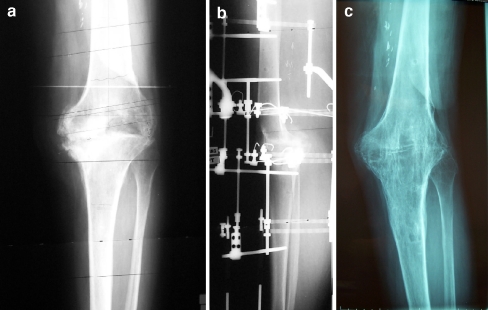
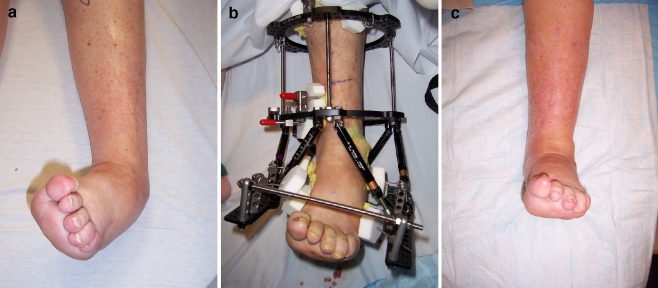
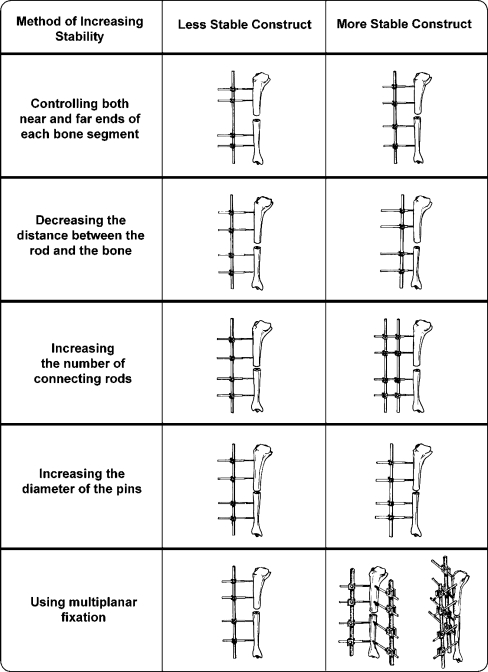
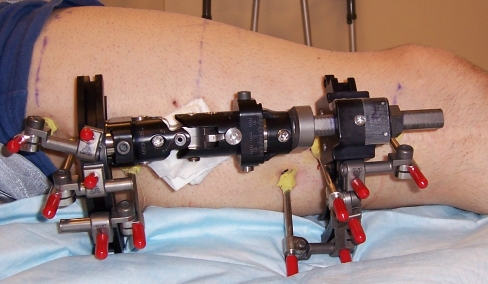
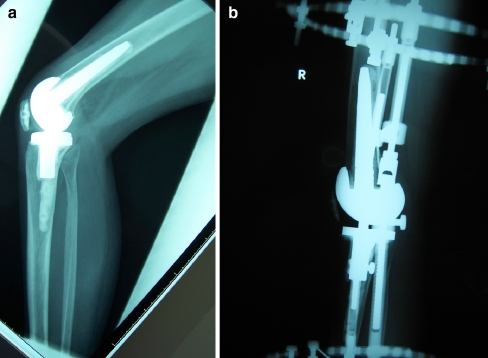
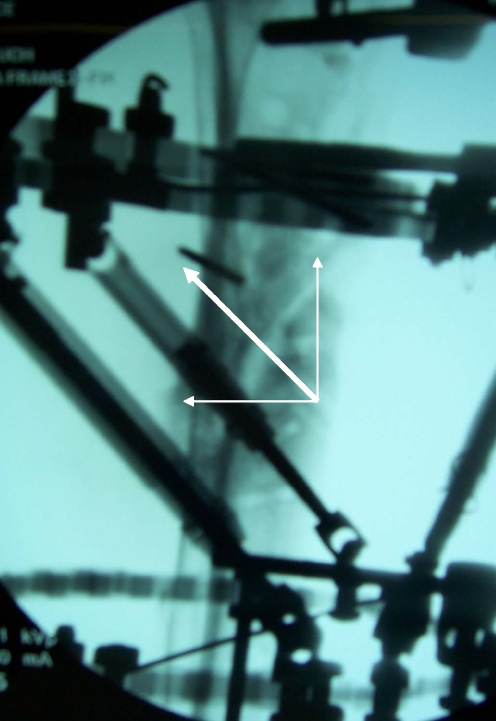
External fixation has evolved from being used primarily as a last resort fixation method to becoming a main stream technique used to treat a myriad of bone and soft tissue pathologies. Techniques in limb reconstruction continue to advance largely as a result of the use of these external devices. A thorough understanding of the biomechanical principles of external fixation is useful for all orthopedic surgeons as most will have to occasionally mount a fixator throughout their career. In this review, various types of external fixators and their common clinical applications are described with a focus on unilateral and circular frames. The biomechanical principles that govern bony and fixator stability are reviewed as well as the recommended techniques for applying external fixators to maximize stability. Additionally, we have illustrated methods for managing patients while they are in the external frames to facilitate function and shorten treatment duration.
Figures














References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '2647333', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/2647333/'}]}
- Behrens F (1989) General theories and principles of external fixation. Clin Orthop 241:15–23 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00003086-199908000-00027', 'is_inner': False, 'url': 'https://doi.org/10.1097/00003086-199908000-00027'}, {'type': 'PubMed', 'value': '10627706', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10627706/'}]}
- Claes L, Heitemeyer U, Krischak G, et al. (1999) Fixation technique influences osteogenesis of comminuted fractures. Clin Orthop 365:221–229 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00005131-200503000-00004', 'is_inner': False, 'url': 'https://doi.org/10.1097/00005131-200503000-00004'}, {'type': 'PubMed', 'value': '15758670', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15758670/'}]}
- Rozbruch SR, Ilizarov S, Blyakher A (2005) Knee arthrodesis with simultaneous lengthening using the Ilizarov method. J Orthop Trauma 19:171–179 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '3514629', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/3514629/'}]}
- Behrens F, Searls K (1986) External fixation of the tibia. Basic concepts and prospective evaluation. J Bone Joint Surg Br 62:246–254 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '6883844', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/6883844/'}]}
- Behrens F, Johnson WD, Koch TW, Kovacevic N (1983) Bending stiffness of unilateral and bilateral fixation frames. Clin Orthop 178:103–110 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
