

Partially overlapping limited anterior and posterior instrumentation for adult thoracolumbar and lumbar scoliosis: a description of novel spinal instrumentation, "the hybrid technique"
- PMID: 18751777
- PMCID: PMC2504101
- DOI: 10.1007/s11420-006-9038-8
Partially overlapping limited anterior and posterior instrumentation for adult thoracolumbar and lumbar scoliosis: a description of novel spinal instrumentation, "the hybrid technique"
Abstract
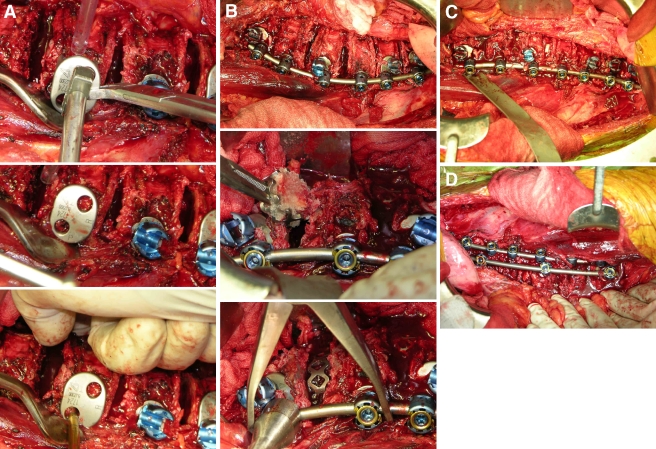
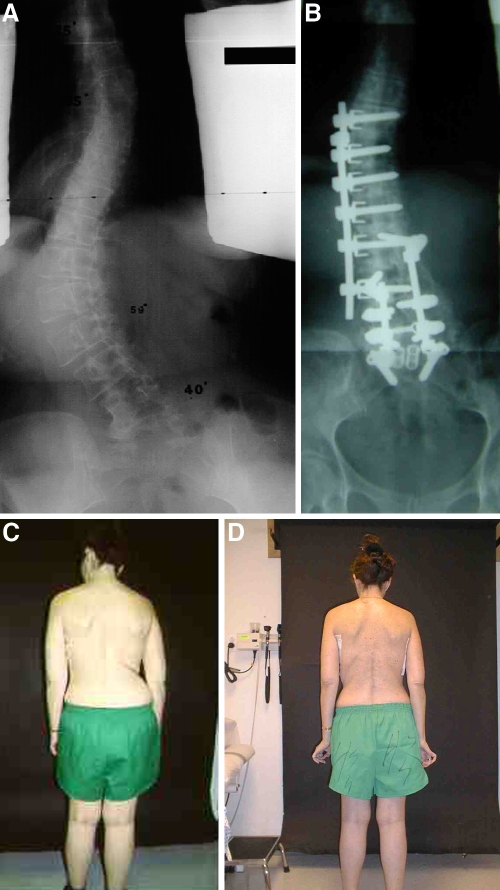
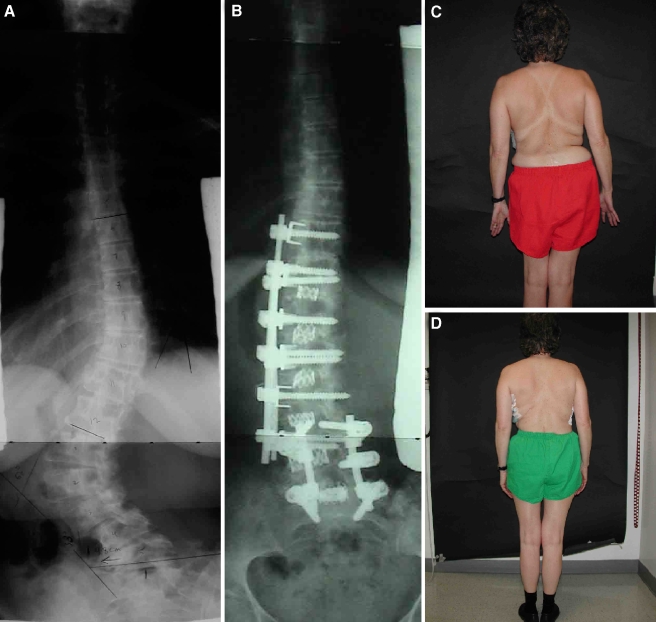
Progressive and/or painful adult spinal deformity in the thoracolumbar and lumbar spine is sometimes treated surgically by long posterior fusions from the thoracic spine down to the pelvis, especially where there is a major thoracic curve component. Recent advances in anterior spinal instrumentation and spinal surgery technique have demonstrated the improved corrective ability offered by anterior stabilization systems, and the added benefit of limiting the number of vertebral fusion levels required for control of the deformity. The "hybrid technique" is a novel use of anterior instrumentation that applies limited anterior instrumentation down to the low lumbar spine (rods and screws), and partially overlapping short-segment posterior instrumentation to the sacrum (pedicle screws and rods). These constructs avoid posterior thoracic instrumentation and fusions, and avoid extension of posterior instrumentation to the pelvis. In the first 10 patients treated using this technique, thoracolumbar and lumbar major curve correction has averaged 71 and 82% in the immediate postoperative period (n = 7), respectively, and 59 and 68% at 2-year follow-up, respectively. The technique is an appealing and attractive alternative for treatment of thoracolumbar and lumbar scoliosis in the adult population, and avoids the requirement for applying spinal fixation to the thoracic spine and the pelvis.
Figures
Similar articles
-
New anterior instrumentation for the management of thoracolumbar and lumbar scoliosis. Application of the Kaneda two-rod system.Spine (Phila Pa 1976). 1996 May 15;21(10):1250-61; discussion 1261-2. doi: 10.1097/00007632-199605150-00021. Spine (Phila Pa 1976). 1996. PMID: 8727201
-
Adult thoracolumbar and lumbar scoliosis treated with long vertebral fusion to the sacropelvis: a comparison between new hybrid selective spinal fusion versus anterior-posterior spinal instrumentation.Spine J. 2014 Apr;14(4):637-45. doi: 10.1016/j.spinee.2013.06.090. Epub 2013 Nov 6. Spine J. 2014. PMID: 24211098
-
Segmental pedicle screw instrumentation in idiopathic thoracolumbar and lumbar scoliosis.Eur Spine J. 2000 Jun;9(3):191-7. doi: 10.1007/s005860000139. Eur Spine J. 2000. PMID: 10905435 Free PMC article. Clinical Trial.
-
Comparative analysis of pedicle screw versus hook instrumentation in posterior spinal fusion of adolescent idiopathic scoliosis.Spine (Phila Pa 1976). 2004 Sep 15;29(18):2040-8. doi: 10.1097/01.brs.0000138268.12324.1a. Spine (Phila Pa 1976). 2004. PMID: 15371706 Review.
-
Treatment of scoliosis in the adult thoracolumbar spine with special reference to fusion to the sacrum.Orthop Clin North Am. 1988 Apr;19(2):371-81. Orthop Clin North Am. 1988. PMID: 3282205 Review.
Cited by
-
Complications in adult spine deformity surgery: a systematic review of the recent literature with reporting of aggregated incidences.Eur Spine J. 2018 Sep;27(9):2272-2284. doi: 10.1007/s00586-018-5535-y. Epub 2018 Mar 1. Eur Spine J. 2018. PMID: 29497853
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00007632-200105010-00012', 'is_inner': False, 'url': 'https://doi.org/10.1097/00007632-200105010-00012'}, {'type': 'PubMed', 'value': '11337635', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11337635/'}]}
- Eck KR, Bridwell KH, Ungacta FF, Riew KD, Lapp MA, Lenke LG, Baldus C, Blanke K (2001) Complications and results of long adult deformity fusions down to l4, l5, and the sacrum. Spine 26(9):E182–E192 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00007632-200204010-00017', 'is_inner': False, 'url': 'https://doi.org/10.1097/00007632-200204010-00017'}, {'type': 'PubMed', 'value': '11923673', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11923673/'}]}
- Emami A, Deviren V, Berven S, Smith JA, Hu SS, Bradford DS (2002) Outcome and complications of long fusions to the sacrum in adult spine deformity: luque-galveston, combined iliac and sacral screws, and sacral fixation. Spine 27(7):776–786 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00007632-200109150-00007', 'is_inner': False, 'url': 'https://doi.org/10.1097/00007632-200109150-00007'}, {'type': 'PubMed', 'value': '11547195', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11547195/'}]}
- Kuklo TR, Bridwell KH, Lewis SJ, Baldus C, Blanke K, Iffrig TM, Lenke LG (2001) Minimum 2-year analysis of sacropelvic fixation and L5–S1 fusion using S1 and iliac screws. Spine 26(18):1976–1983 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/01.brs.0000197193.81296.f1', 'is_inner': False, 'url': 'https://doi.org/10.1097/01.brs.0000197193.81296.f1'}, {'type': 'PubMed', 'value': '16449903', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16449903/'}]}
- Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C (2006) Minimum 5-year analysis of L5–S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine 31(3):303–308 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '1523506', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/1523506/'}]}
- McCord DH, Cunningham BW, Shono Y, Myers JJ, McAfee PC (1992) Biomechanical analysis of lumbosacral fixation. Spine 17(8 Suppl):S235–S243 - PubMed
LinkOut - more resources
Full Text Sources
