

Hip arthroscopy update
- PMID: 18751808
- PMCID: PMC2504137
- DOI: 10.1007/s11420-005-0105-3
Hip arthroscopy update
Abstract
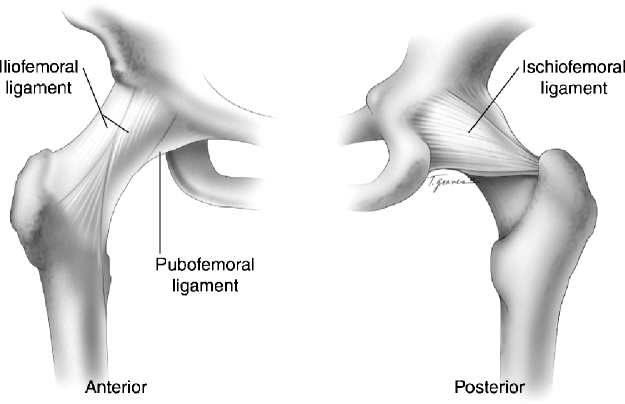
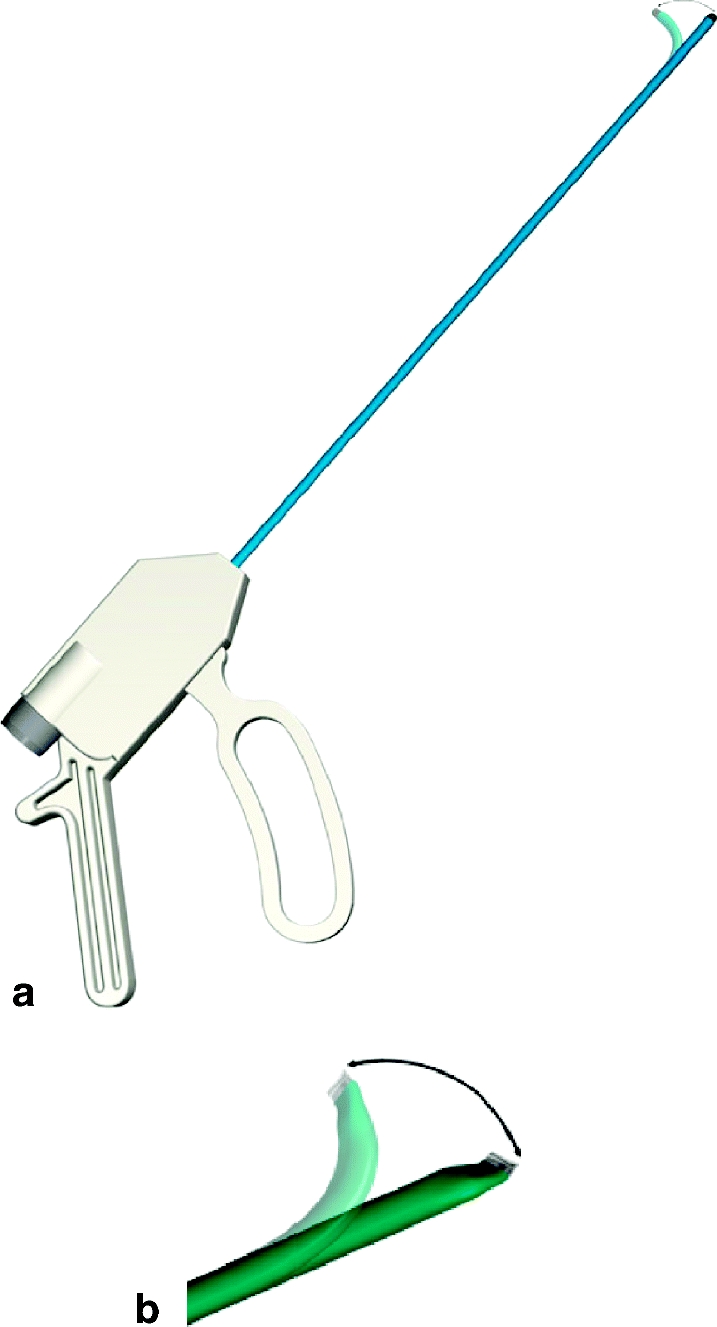
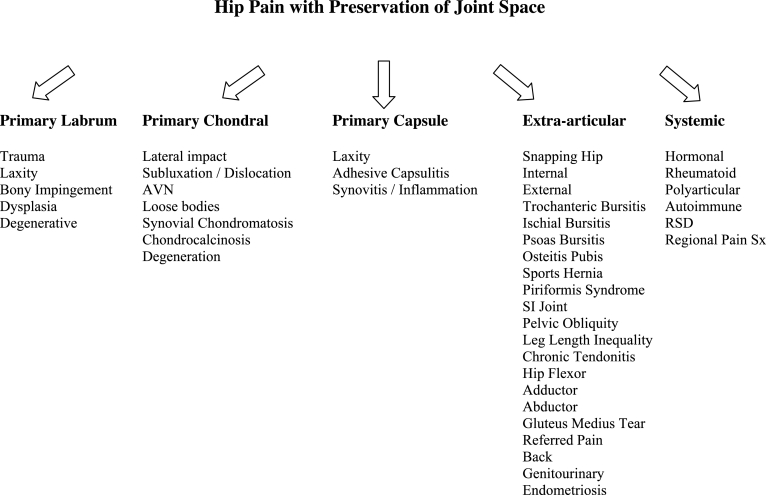
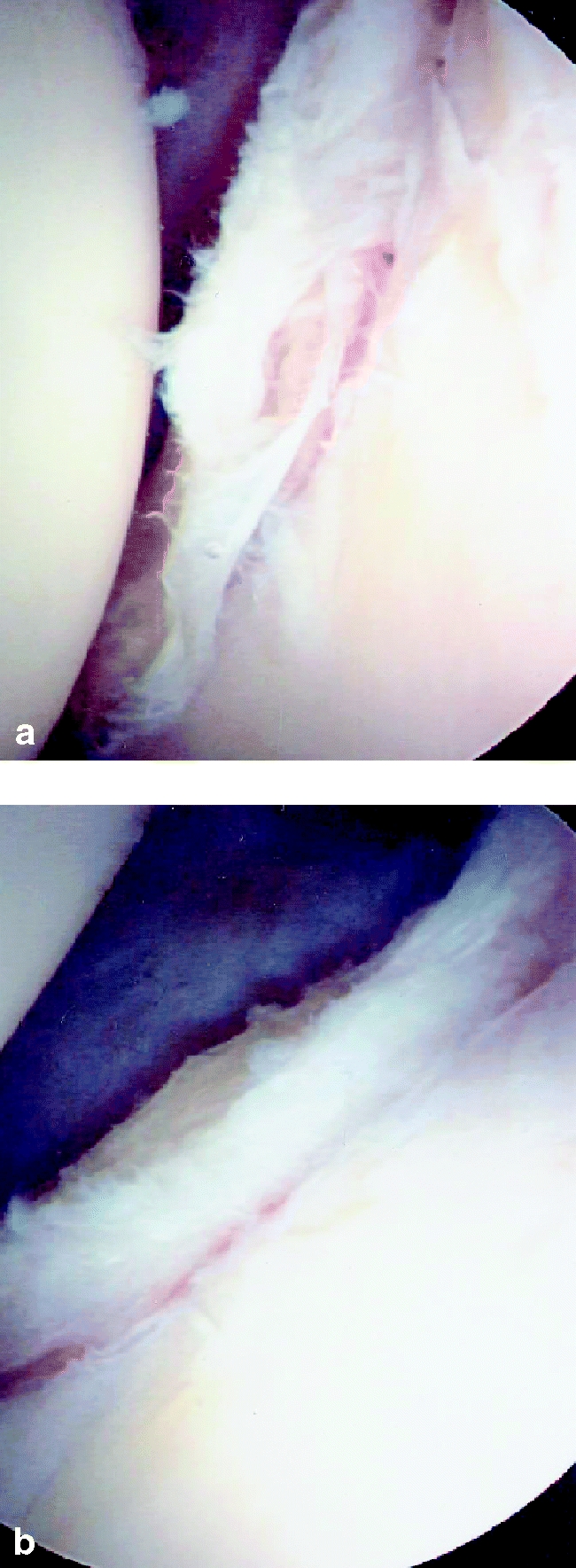
The management of hip injuries in the athlete has evolved significantly in the past few years with the advancement of arthroscopic techniques. The application of minimally invasive surgical techniques has facilitated relatively rapid returns to sporting activity in recreational and elite athletes alike. Recent advancements in both hip arthroscopy and magnetic resonance imaging have elucidated several sources of intraarticular pathology that result in chronic and disabling hip symptoms. Many of these conditions were previously unrecognized and thus, left untreated. Current indications for hip arthroscopy include management of labral tears, osteoplasty for femoroacetabular impingement, thermal capsulorrhaphy and capsular plication for subtle rotational instability and capsular laxity, lateral impact injury and chondral lesions, osteochondritis dissecans, ligamentum teres injuries, internal and external snapping hip, removal of loose bodies, synovial biopsy, subtotal synovectomy, synovial chondromatosis, infection, and certain cases of mild to moderate osteoarthritis with associated mechanical symptoms. In addition, patients with long-standing, unresolved hip joint pain and positive physical findings may benefit from arthroscopic evaluation. Patients with reproducible symptoms and physical findings that reveal limited functioning, and who have failed an adequate trial of conservative treatment will have the greatest likelihood of success after surgical intervention. Strict attention to thorough diagnostic examination, detailed imaging, and adherence to safe and reproducible surgical techniques, as described in this review, are essential for the success of this procedure.
Figures


References
-
- Allen WC, Cope R. Coxa saltans: the snapping hip revisited. J Am Acad Orthop Surg. 1995;3(5):303–308. - PubMed
-
- Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop. 2004;418:67–73. - PubMed
-
- Bharam S, Draovitch P, Fu F, Philippon MJ (2002) Return to competition in professional athletes with traumatic labral tears ofthe hip. In: 28th Annual Meeting of American Orthopaedic Society of Sports Medicine, Orlando, Fl
-
- Bharam S, Kandemir V, Draovitch P, Fu F, Philippon MJ (2003) Management of hip injuries in PGA golfers with arthroscopy. In: 70th Annual Meeting of American Academy of OrthopaedicSurgeons, New Orleans, LA, p 485
-
- Byrd JW. Hip arthroscopy in athletes. Instr Course Lect. 2003;52:701–709. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
