

Ketamine as an adjunct to postoperative pain management in opioid tolerant patients after spinal fusions: a prospective randomized trial
- PMID: 18751864
- PMCID: PMC2504281
- DOI: 10.1007/s11420-007-9069-9
Ketamine as an adjunct to postoperative pain management in opioid tolerant patients after spinal fusions: a prospective randomized trial
Abstract
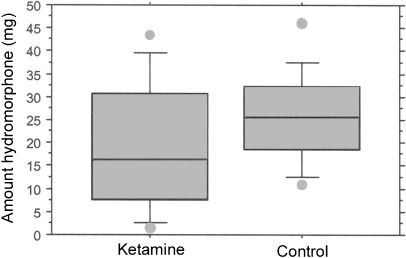
Management of acute postoperative pain is challenging, particularly in patients with preexisting narcotic dependency. Ketamine has been used at subanesthetic doses as a N-methyl D-aspartate (NMDA) receptor antagonist to block the processing of nociceptive input in chronic pain syndromes. This prospective randomized study was designed to assess the use of ketamine as an adjunct to acute pain management in narcotic tolerant patients after spinal fusions. Twenty-six patients for 1-2 level posterior lumbar fusions with segmental instrumentation were randomly assigned to receive ketamine or act as a control. Patients in the ketamine group received 0.2 mg/kg on induction of general anesthesia and then 2 mcg kg(-1) hour(-1) for the next 24 hours. Patients were extubated in the operating room and within 15 minutes of arriving in the Post Anesthesia Care Unit (PACU) were started on intravenous patient-controlled analgesia (PCA) hydromorphone without a basal infusion. Patients were assessed for pain (numerical rating scale [NRS]), narcotic use, level of sedation, delirium, and physical therapy milestones until discharge. The ketamine group had significantly less pain during their first postoperative hour in the PACU (NRS 4.8 vs 8.7) and continued to have less pain during the first postoperative day at rest (3.6 vs 5.5) and with physical therapy (5.6 vs 8.0). Three patients in the control group failed PCA pain management and were converted to intravenous ketamine infusions when their pain scores improved. Patients in the ketamine group required less hydromorphone than the control group, but the differences were not significant. Subanesthetic doses of ketamine reduced postoperative pain in narcotic tolerant patients undergoing posterior spine fusions.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
