

Development of antibodies to PspA families 1 and 2 in children after exposure to Streptococcus pneumoniae
- PMID: 18753341
- PMCID: PMC2565922
- DOI: 10.1128/CVI.00181-08
Development of antibodies to PspA families 1 and 2 in children after exposure to Streptococcus pneumoniae
Abstract
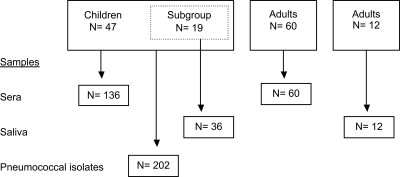
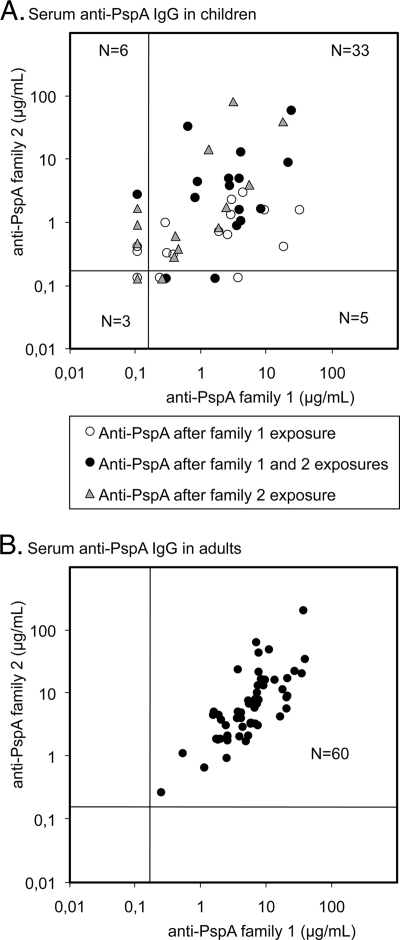
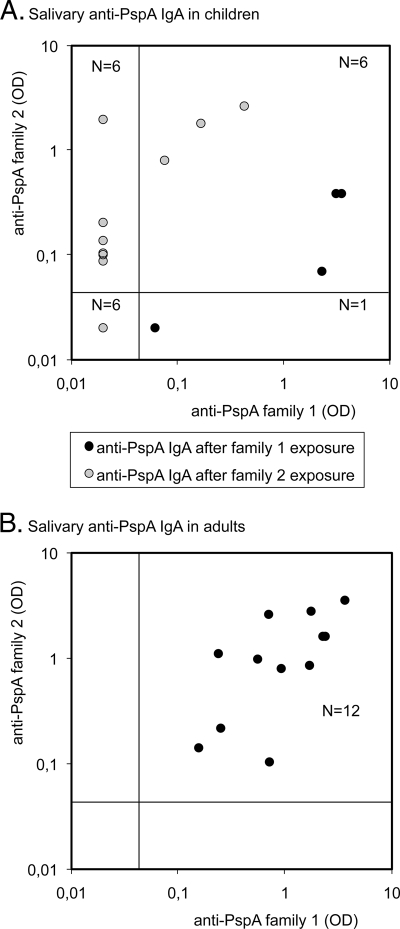
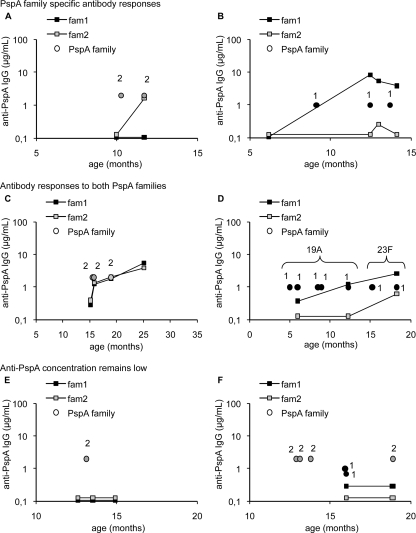
Pneumococcal surface protein A (PspA) is an important virulence factor of Streptococcus pneumoniae. PspA exists as two major families, which include variable but serologically cross-reactive proteins. Previous studies with a family 1 PspA antigen suggested that children develop low concentrations of anti-PspA after pneumococcal carriage or infection. In this study, antibody to PspA families 1 and 2 was measured by an enzyme immunoassay of the serum and saliva of children with a history of culture-proven pneumococcal colonization and/or acute otitis media and in the serum and saliva of adults. The PspA families of the pneumococcal strains isolated from children were determined. The majority of the children had high serum and salivary anti-PspA concentrations to the PspA family they had encountered and low concentrations to the other, whereas adults had high antibody concentrations to both PspA families, both in serum and in saliva. The results suggest that children have a relatively family-specific antibody response to the PspA family they have been exposed to and that any PspA vaccine for children should contain members of both major PspA families.
Figures
References
-
- Briles, D. E., E. Ades, J. C. Paton, J. S. Sampson, G. M. Carlone, R. C. Huebner, A. Virolainen, E. Swiatlo, and S. K. Hollingshead. 2000. Intranasal immunization of mice with a mixture of the pneumococcal proteins PsaA and PspA is highly protective against nasopharyngeal carriage of Streptococcus pneumoniae. Infect. Immun. 68:796-800. - PMC - PubMed
-
- Briles, D. E., S. K. Hollingshead, J. King, A. Swift, P. A. Braun, M. K. Park, L. M. Ferguson, M. H. Nahm, and G. S. Nabors. 2000. Immunization of humans with recombinant pneumococcal surface protein A (rPspA) elicits antibodies that passively protect mice from fatal infection with Streptococcus pneumoniae bearing heterologous PspA. J. Infect. Dis. 182:1694-1701. - PubMed
-
- Briles, D. E., S. K. Hollingshead, J. C. Paton, E. W. Ades, L. Novak, F. W. van Ginkel, and W. H. Benjamin, Jr. 2003. Immunizations with pneumococcal surface protein A and pneumolysin are protective against pneumonia in a murine model of pulmonary infection with Streptococcus pneumoniae. J. Infect. Dis. 188:339-348. - PubMed
-
- Briles, D. E., S. K. Hollingshead, E. Swiatlo, A. Brooks-Walter, A. Szalai, A. Virolainen, L. S. McDaniel, K. A. Benton, P. White, K. Prellner, A. Hermansson, P. C. Aerts, H. Van Dijk, and M. J. Crain. 1997. PspA and PspC: their potential for use as pneumococcal vaccines. Microb. Drug Resist. 3:401-408. - PubMed
-
- Briles, D. E., R. C. Tart, H. Y. Wu, B. A. Ralph, M. W. Russell, and L. S. McDaniel. 1996. Systemic and mucosal protective immunity to pneumococcal surface protein A. Ann. N. Y. Acad. Sci. 797:118-126. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
