

Baseline renal insufficiency and risk of death among HIV-infected adults on antiretroviral therapy in Lusaka, Zambia
- PMID: 18753939
- PMCID: PMC2649719
- DOI: 10.1097/QAD.0b013e328307a051
Baseline renal insufficiency and risk of death among HIV-infected adults on antiretroviral therapy in Lusaka, Zambia
Abstract
Objective: To examine the association between baseline renal insufficiency and mortality among adults initiating antiretroviral therapy (ART) in an urban African setting.
Design: Open cohort evaluation.
Methods: We examined mortality according to baseline renal function among adults initiating ART in Lusaka, Zambia. Renal function was assessed by the Cockcroft-Gault method, the Modification of Diet in Renal Disease equation, and serum creatinine.
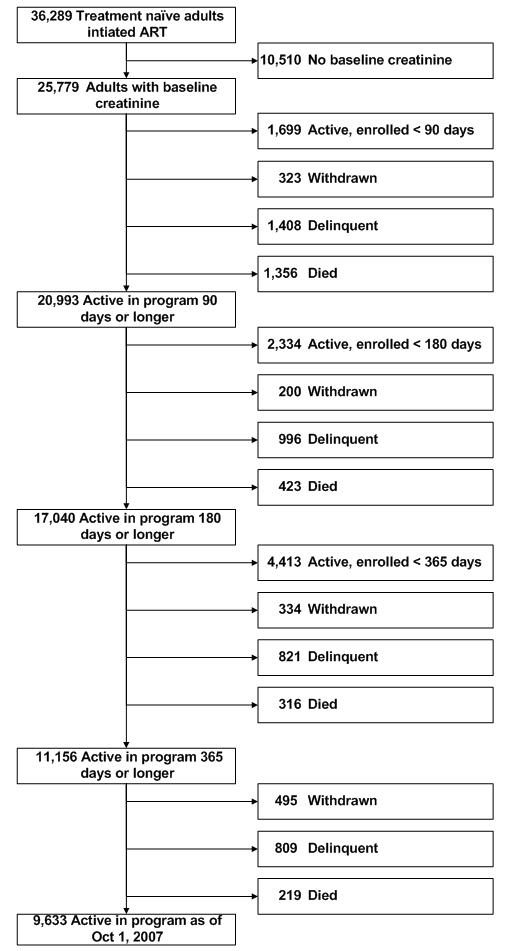
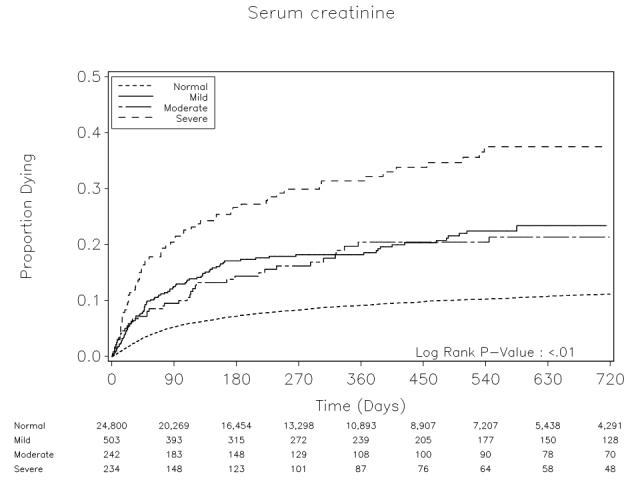
Results: From April 2004 to September 2007, 25 779 individuals started ART with an available creatinine measurement at baseline. When creatinine clearance was calculated by the Cockcroft-Gault method, 8456 (33.5%) had renal insufficiency: 73.5% were mild (60-89 ml/min), 23.4% moderate (30-59 ml/min), and 3.1% severe (<30 ml/min). Risk for mortality at or before 90 days was elevated for those with mildly [adjusted hazard ratio (AHR)(1/4)1.7; 95% confidence interval (95% CI)(1/4)1.5-1.9], moderately (AHR(1/4)2.3; 95% CI(1/4)2.0-2.7), and severely (AHR(1/4)4.3; 95% CI(1/4)3.1-5.5) reduced creatinine clearance. Mild (AHR(1/4)1.4; 95% CI(1/4)1.2-1.6), moderate (AHR(1/4)1.9; 95% CI(1/4)1.5-2.3), and severe (AHR(1/4)3.6; 95% CI(1/4) 2.4-5.5) insufficiency were also associated with increased mortality after 90 days, when compared with those with normal renal function. Trends were similar when renal function was estimated with Modification of Diet in Renal Disease or serum creatinine.
Conclusion: Renal insufficiency at time of ART initiation was prevalent and associated with increased mortality risk among adults in this population. These results have particular relevance for settings like Zambia, where tenofovir--a drug with known nephrotoxicity--has been adopted as part of first-line therapy. This emphasizes the need for resource-appropriate screening algorithms for renal disease, both as part of ART eligibility and pretreatment assessment.


References
-
- Szczech LA. Renal diseases associated with human immunodeficiency virus infection: epidemiology, clinical course, and management. Clin Infect Dis. 2001;33:115–119. - PubMed
-
- Ross MJ, Fan C, Ross MD, Chu TH, Shi Y, Kaufman L, et al. HIV-1 infection initiates an inflammatory cascade in human renal tubular epithelial cells. J Acquir Immune Defic Syndr. 2006;42:1–11. - PubMed
-
- Weiner NJ, Goodman JW, Kimmel PL. The HIV-associated renal diseases: current insight into pathogenesis and treatment. Kidney Int. 2003;63:1618–1631. - PubMed
-
- Franceschini N, Napravnik S, Finn WF, Szczech LA, Eron JJ., Jr Immunosuppression, hepatitis C infection, and acute renal failure in HIV-infected patients. J Acquir Immune Defic Syndr. 2006;42:368–372. - PubMed
-
- Glassock RJ, Cohen AH, Danovitch G, Parsa KP. Human immunodeficiency virus (HIV) infection and the kidney. Ann Intern Med. 1990;112:35–49. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
