

Rituximab in combination with high-dose methylprednisolone for the treatment of fludarabine refractory high-risk chronic lymphocytic leukemia
- PMID: 18754025
- PMCID: PMC5289283
- DOI: 10.1038/leu.2008.214
Rituximab in combination with high-dose methylprednisolone for the treatment of fludarabine refractory high-risk chronic lymphocytic leukemia
Abstract
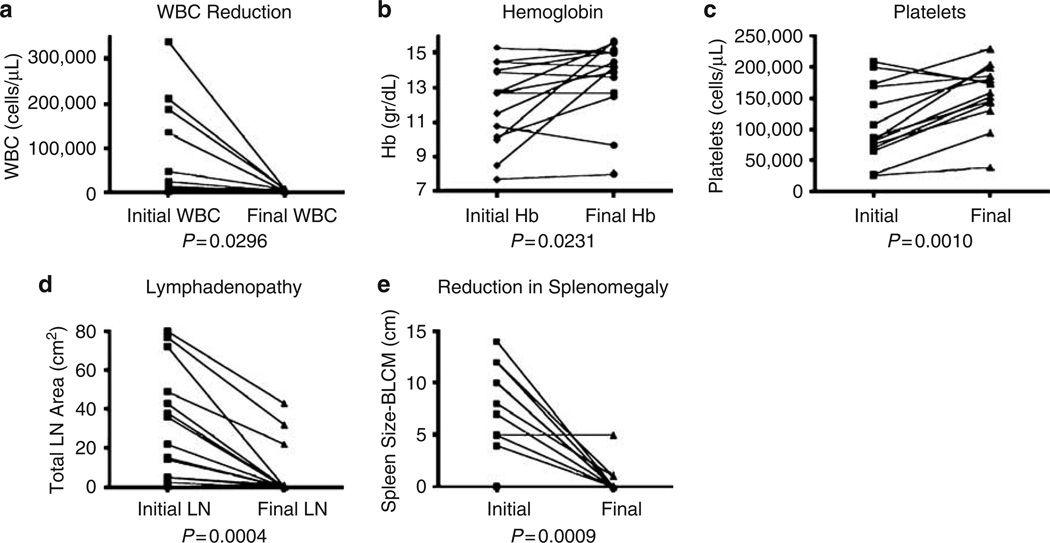
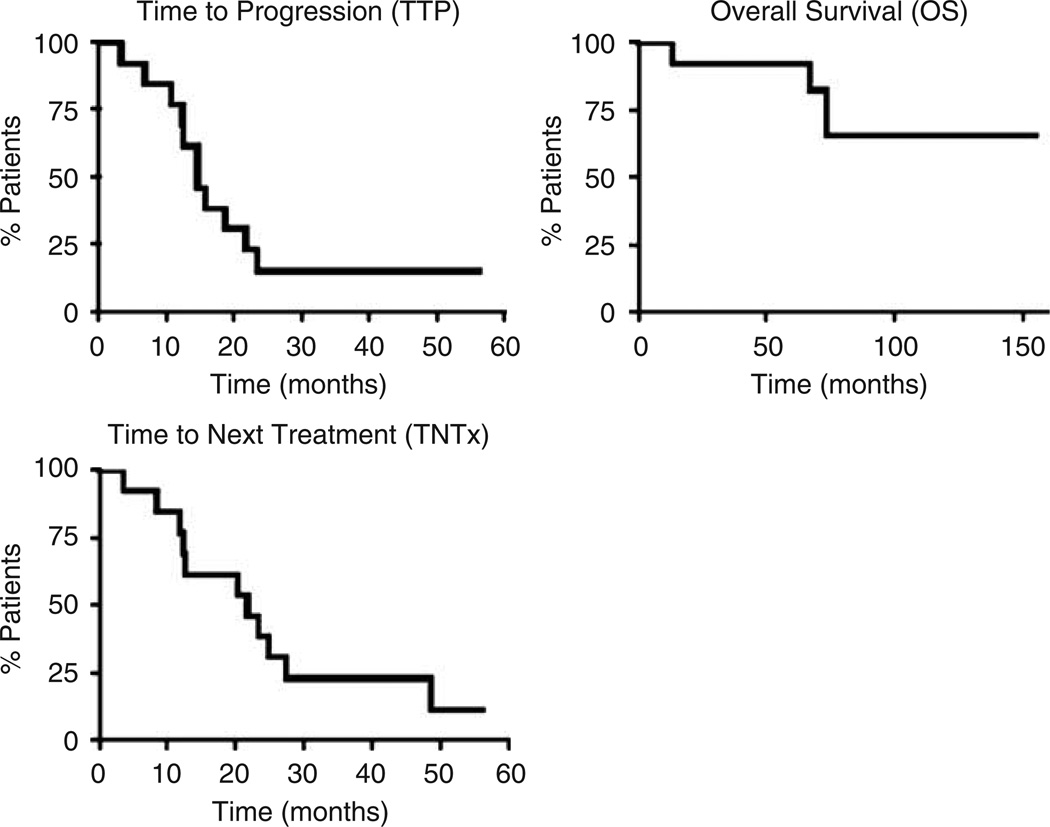
We examined the clinical response of fludarabine-refractory CLL patients treated with high-dose methylprednisolone (HDMP) and rituximab. Fourteen patients were treated with three cycles of rituximab (375 mg/m(2) weekly for 4 weeks) in combination with HDMP (1 gm/m(2) daily for 5 days). All patients were refractory to fludarabine and 86% had high-risk disease by the modified Rai classification. In all, 79% of the patients had CLL cells that expressed ZAP-70 and three patients had poor prognostic cytogenetics. The overall response rate was 93% and the complete remission rate was 36%. The median time-to-progression was 15 months and the median time-to-next treatment was 22 months. Median survival has not been reached after a median follow up of 40 months. Four patients have died of progressive disease. Patients tolerated the treatment well and serious adverse events were rare. This allowed patients to receive all planned treatments on schedule with no dose modifications. All but one patient responded to treatment and the overall survival and time-to-progression were superior to those of other published salvage regimens.
Figures
References
-
- Wierda W, O’Brien S, Wen S, Faderl S, Garcia-Manero G, Thomas D, et al. Chemoimmunotherapy with fludarabine, cyclophosphamide, and rituximab for relapsed and refractory chronic lymphocytic leukemia. J Clin Oncol. 2005;23:4070–4078. - PubMed
-
- Bosch F, Ferrer A, Lopez-Guillermo A, Gine E, Bellosillo B, Villamor N, et al. Fludarabine, cyclophosphamide and mitoxantrone in the treatment of resistant or relapsed chronic lymphocytic leukaemia. Br J Haematol. 2002;119:976–984. - PubMed
-
- Keating MJ, Flinn I, Jain V, Binet JL, Hillmen P, Byrd J, et al. Therapeutic role of alemtuzumab (Campath-1H) in patients who have failed fludarabine: results of a large International Study. Blood. 2002;99:3554–3561. - PubMed
-
- Rai KR, Freter CE, Mercier RJ, Cooper MR, Mitchell BS, Stadtmauer EA, et al. Alemtuzumab in previously treated chronic lymphocytic leukemia patients who also had received fludarabine. J Clin Oncol. 2002;20:3891–3897. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
