

Type 1 helper T cells and FoxP3-positive T cells in HIV-tuberculosis-associated immune reconstitution inflammatory syndrome
- PMID: 18755923
- PMCID: PMC2643222
- DOI: 10.1164/rccm.200806-858OC
Type 1 helper T cells and FoxP3-positive T cells in HIV-tuberculosis-associated immune reconstitution inflammatory syndrome
Abstract
Rationale: Tuberculosis-associated immune reconstitution inflammatory syndrome (TB-IRIS) induced by combination antiretroviral therapy (cART) has been attributed to dysregulated expansion of tuberculin PPD-specific IFN-gamma-secreting CD4(+) T cells.
Objectives: To investigate the role of type 1 helper T cell expansions and regulatory T cells in HIV-TB IRIS.
Methods: Longitudinal and cross-sectional studies of Mycobacterium tuberculosis-specific IFN-gamma enzyme-linked immunospot responses and flow cytometric analysis of blood cells from a total of 129 adults with HIV-1-associated tuberculosis, 98 of whom were prescribed cART.
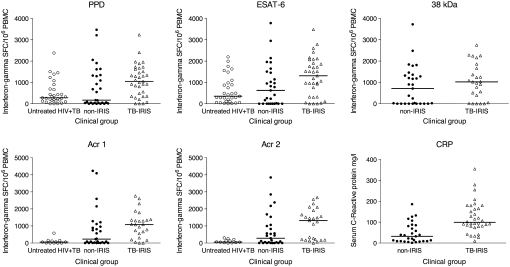
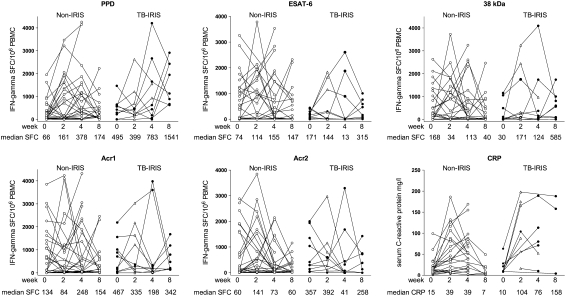
Measurements and main results: In cross-sectional analysis the frequency of IFN-gamma-secreting T cells recognizing early secretory antigenic target (ESAT)-6, alpha-crystallins 1 and 2, and PPD of M. tuberculosis was higher in patients with TB-IRIS than in similar patients treated for both HIV-1 and tuberculosis who did not develop IRIS (non-IRIS; P <or= 0.03). The biggest difference was in the recognition of alpha-crystallin molecules: peptide mapping indicated a polyclonal response. Flow cytometric analysis indicated equal proportions of CD4(+) and CD8(+) cells positive for activation markers HLA-DR and CD71 in both patients with TB-IRIS and non-IRIS patients. The percentage of CD4(+) cells positive for FoxP3 (Forkhead box P3) was low in both groups (TB-IRIS, 5.3 +/- 4.5; non-IRIS, 2.46 +/- 2.46; P = 0.13). Eight weeks of longitudinal analysis of patients with tuberculosis who were starting cART showed dynamic changes in antigen-specific IFN-gamma-secreting T cells in both the TB-IRIS and non-IRIS groups: the only significant trend was an increased response to PPD in the TB-IRIS group (P = 0.041).
Conclusions: There is an association between helper T-cell type 1 expansions and TB-IRIS, but the occurrence of similar expansions in non-IRIS brings into question whether these are causal. The defect in immune regulation responsible for TB-IRIS remains to be fully elucidated.
Figures

References
-
- Maartens G, Wilkinson RJ. Tuberculosis. Lancet 2007;370:2030–2043. - PubMed
-
- Badri M, Wilson D, Wood R. Effect of highly active antiretroviral therapy on incidence of tuberculosis in South Africa: a cohort study. Lancet 2002;359:2059–2064. - PubMed
-
- Lawn S, Badri M, Wood R. Tuberculosis among HIV-infected patients receiving HAART: long term incidence and risk factors in a South African cohort. AIDS 2005;19:2109–2116. - PubMed
-
- Autran B, Carcelain G, Li TS, Blanc C, Mathez D, Tubiana R, Katlama C, Debre P, Leibowitch J. Positive effects of combined antiretroviral therapy on CD4+ T cell homeostasis and function in advanced HIV disease. Science 1997;277:112–116. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
