

Assessing validity of ICD-9-CM and ICD-10 administrative data in recording clinical conditions in a unique dually coded database
- PMID: 18756617
- PMCID: PMC2517283
- DOI: 10.1111/j.1475-6773.2007.00822.x
Assessing validity of ICD-9-CM and ICD-10 administrative data in recording clinical conditions in a unique dually coded database
Abstract
Objective: The goal of this study was to assess the validity of the International Classification of Disease, 10th Version (ICD-10) administrative hospital discharge data and to determine whether there were improvements in the validity of coding for clinical conditions compared with ICD-9 Clinical Modification (ICD-9-CM) data.
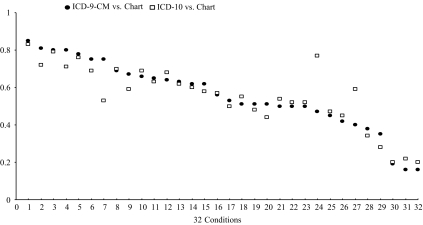
Methods: We reviewed 4,008 randomly selected charts for patients admitted from January 1 to June 30, 2003 at four teaching hospitals in Alberta, Canada to determine the presence or absence of 32 clinical conditions and to assess the agreement between ICD-10 data and chart data. We then re-coded the same charts using ICD-9-CM and determined the agreement between the ICD-9-CM data and chart data for recording those same conditions. The accuracy of ICD-10 data relative to chart data was compared with the accuracy of ICD-9-CM data relative to chart data.
Results: Sensitivity values ranged from 9.3 to 83.1 percent for ICD-9-CM and from 12.7 to 80.8 percent for ICD-10 data. Positive predictive values ranged from 23.1 to 100 percent for ICD-9-CM and from 32.0 to 100 percent for ICD-10 data. Specificity and negative predictive values were consistently high for both ICD-9-CM and ICD-10 databases. Of the 32 conditions assessed, ICD-10 data had significantly higher sensitivity for one condition and lower sensitivity for seven conditions relative to ICD-9-CM data. The two databases had similar sensitivity values for the remaining 24 conditions.
Conclusions: The validity of ICD-9-CM and ICD-10 administrative data in recording clinical conditions was generally similar though validity differed between coding versions for some conditions. The implementation of ICD-10 coding has not significantly improved the quality of administrative data relative to ICD-9-CM. Future assessments like this one are needed because the validity of ICD-10 data may get better as coders gain experience with the new coding system.
Figures

References
-
- Anderson RN, Rosenberg HM. Disease Classification: Measuring the Effect of the Tenth Revision of the International Classification of Diseases on Cause-of-Death Data in the United States. Statistics in Medicine. 2003;22:1551–70. - PubMed
-
- Best WR, Khuri SF, Phelan M, Hur K, Henderson WG, Demakis JG, Daley J. Identifying Patient Preoperative Risk Factors and Postoperative Adverse Events in Administrative Databases: Results from the Department of Veterans Affairs National Surgical Quality Improvement Program. Journal of American College of Surgeons. 2002;194:257–66. - PubMed
-
- Canadian Institute for Health Information. International Statistical Classification of Diseases and Related Health Problems Tenth Revision, Canada [ICD-10-CA] Ottawa, ON: Canadian Institute for Health Information; 2003.
-
- Canadian Institute for Health Information. Canadian Coding Standards for ICD-10-CA and CCI for 2007. Ottawa: Canadian Institute of Health Information; 2007.
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. Journal of Chronic Diseases. 1987;40:373–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
